Das könnte Ihnen auch gefallen
- Bone-Anchored Hearing Aid (BAHA) : Indications, Functional Results, and Comparison With Reconstructive Surgery of The EarDokument7 SeitenBone-Anchored Hearing Aid (BAHA) : Indications, Functional Results, and Comparison With Reconstructive Surgery of The EarShanaz KanandaNoch keine Bewertungen
- Healthcare 11 00676 v2Dokument10 SeitenHealthcare 11 00676 v2andiNoch keine Bewertungen
- Genetic Variants in The Peripheral Auditory System Significan 2017 Hearing RDokument5 SeitenGenetic Variants in The Peripheral Auditory System Significan 2017 Hearing RJuan Sebas VizueteNoch keine Bewertungen
- Baha in Japan 2008Dokument4 SeitenBaha in Japan 2008pijas2980Noch keine Bewertungen
- Clinical Oral Implants Res - 2009 - Serino - Peri Implantitis in Partially Edentulous Patients Association With InadequateDokument6 SeitenClinical Oral Implants Res - 2009 - Serino - Peri Implantitis in Partially Edentulous Patients Association With InadequateNourhan IbrahimNoch keine Bewertungen
- Stapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesDokument10 SeitenStapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesLuis De jesus SolanoNoch keine Bewertungen
- Neurotology Audiology: ProceedingsDokument5 SeitenNeurotology Audiology: ProceedingsLucia Rodriguez GarciaNoch keine Bewertungen
- Batson2017 OtosclerosisDokument6 SeitenBatson2017 OtosclerosisnuhajazminNoch keine Bewertungen
- 1 PBDokument7 Seiten1 PBHigherNoch keine Bewertungen
- J-Stage KimDokument6 SeitenJ-Stage Kimkelompok cNoch keine Bewertungen
- 2019 - Hakansson Et Al (BC Device Follow Up)Dokument11 Seiten2019 - Hakansson Et Al (BC Device Follow Up)overkindNoch keine Bewertungen
- Patient Benefit From Cochlear Implantation in Single-Sided Deafness: A 1-Year Follow-UpDokument5 SeitenPatient Benefit From Cochlear Implantation in Single-Sided Deafness: A 1-Year Follow-UpRonald Rey MenorNoch keine Bewertungen
- Varadarajan Et Al 2020 Evolving Criteria For Adult and Pediatric Cochlear ImplantationDokument7 SeitenVaradarajan Et Al 2020 Evolving Criteria For Adult and Pediatric Cochlear ImplantationCoAsst MuhammadNuhAlhudawyNoch keine Bewertungen
- Effect of Cochlear Implantation On Quality of Life in Adults With Unilateral Hearing LossDokument13 SeitenEffect of Cochlear Implantation On Quality of Life in Adults With Unilateral Hearing LossRonald Rey MenorNoch keine Bewertungen
- BAHA: Bone-Anchored Hearing Aid Abdulrahman HagrDokument12 SeitenBAHA: Bone-Anchored Hearing Aid Abdulrahman HagrDavidBrionesNoch keine Bewertungen
- These Archivage 3369507oDokument143 SeitenThese Archivage 3369507oKennedy NgoseyweNoch keine Bewertungen
- Bag Uley 2006Dokument2 SeitenBag Uley 2006Harshit AmbeshNoch keine Bewertungen
- First Premolar Extraction Effects On Upper Airway Dimension in Bimaxillary Proclination PatientsDokument7 SeitenFirst Premolar Extraction Effects On Upper Airway Dimension in Bimaxillary Proclination PatientsJean-Philippe MercierNoch keine Bewertungen
- Indications For Cochlear ImplantsDokument12 SeitenIndications For Cochlear Implantscristina georgianaNoch keine Bewertungen
- Omori 2019Dokument11 SeitenOmori 2019Maisely Fabiluz Galindo GomezNoch keine Bewertungen
- Articulo Mordida ProfundaDokument6 SeitenArticulo Mordida ProfundaCristina TelloNoch keine Bewertungen
- Effects of Cochlear Implantation on Binaural Hearing in Adults With Unilateral Hearing LossDokument40 SeitenEffects of Cochlear Implantation on Binaural Hearing in Adults With Unilateral Hearing LossAnggita PuspitasariNoch keine Bewertungen
- Life 12 00137 v2Dokument12 SeitenLife 12 00137 v2tia tamaraNoch keine Bewertungen
- Combined OAE and AABR Approach For Newborn Hearing ScreeningDokument31 SeitenCombined OAE and AABR Approach For Newborn Hearing ScreeningCrl IwnNoch keine Bewertungen
- Acs 2 PDFDokument10 SeitenAcs 2 PDFCarolina UrrutiaNoch keine Bewertungen
- Cochlear Implantation in Postlingually Deaf Adults Is Time-Sensitive Towards Positive Outcome: Prediction Using Advanced Machine Learning TechniquesDokument9 SeitenCochlear Implantation in Postlingually Deaf Adults Is Time-Sensitive Towards Positive Outcome: Prediction Using Advanced Machine Learning TechniquesXilena HerreraNoch keine Bewertungen
- Incidence of Developing Contralateral M Enie're's Disease in Patients Undergoing Transmastoid Labyrinthectomy For Unilateral M Enie're's DiseaseDokument4 SeitenIncidence of Developing Contralateral M Enie're's Disease in Patients Undergoing Transmastoid Labyrinthectomy For Unilateral M Enie're's DiseaseNoviTrianaNoch keine Bewertungen
- Dental Arch Changes After Open Bite Treatment With SpursDokument11 SeitenDental Arch Changes After Open Bite Treatment With SpursDavid TantaleánNoch keine Bewertungen
- PEÑARANDADokument8 SeitenPEÑARANDAAlejandroNoch keine Bewertungen
- Zobay Et Al 2023 Fitting A Hearing Aid On The Better Ear Worse Ear or Both Associations of Hearing Aid FittingDokument13 SeitenZobay Et Al 2023 Fitting A Hearing Aid On The Better Ear Worse Ear or Both Associations of Hearing Aid FittingAlex A.Noch keine Bewertungen
- JConservDent223313-489526 000809Dokument5 SeitenJConservDent223313-489526 000809poojaNoch keine Bewertungen
- Differences in Finished Case Quality Between Invisalign and Traditional Fixed ApplianceDokument7 SeitenDifferences in Finished Case Quality Between Invisalign and Traditional Fixed Applianceluthfi fernandaNoch keine Bewertungen
- INGLES - Medical, Technical and Audiological Outcomes of Hearing RehabilitationDokument9 SeitenINGLES - Medical, Technical and Audiological Outcomes of Hearing RehabilitationWilliam Alexander Guzman MartinNoch keine Bewertungen
- Learning, Memory, and Cognitive Processes in Deaf Children Following Cochlear ImplantationDokument50 SeitenLearning, Memory, and Cognitive Processes in Deaf Children Following Cochlear ImplantationSoporte CeffanNoch keine Bewertungen
- Acs 4Dokument25 SeitenAcs 4Carolina UrrutiaNoch keine Bewertungen
- INGLES - Active Transcutaneous Bone Conduction Hearing ImplantsDokument19 SeitenINGLES - Active Transcutaneous Bone Conduction Hearing ImplantsWilliam Alexander Guzman MartinNoch keine Bewertungen
- 1 s2.0 S2095881118300611 Main 2Dokument5 Seiten1 s2.0 S2095881118300611 Main 2Delia RasmawatiNoch keine Bewertungen
- Functional Loss After Meningitis-Evaluation of Vestibular Function in Patients With Postmeningitic Hearing LossDokument10 SeitenFunctional Loss After Meningitis-Evaluation of Vestibular Function in Patients With Postmeningitic Hearing LossJuan Camilo Rubiano CuellarNoch keine Bewertungen
- Tinnitus and Hearing Survey Cultural Adaptati 2021 Brazilian Journal of OtoDokument7 SeitenTinnitus and Hearing Survey Cultural Adaptati 2021 Brazilian Journal of OtoNavin SNNoch keine Bewertungen
- Blamey 2015 Niv. 3Dokument11 SeitenBlamey 2015 Niv. 3sainath.vidya0309Noch keine Bewertungen
- Anesthetic Efficacy of Buccal Infiltration Articaine Versus Lidocaine For Extraction of Primary Molar TeethDokument5 SeitenAnesthetic Efficacy of Buccal Infiltration Articaine Versus Lidocaine For Extraction of Primary Molar TeethFabro BianNoch keine Bewertungen
- 2023 Apr - Pre Clinical Evaluation of APrevent VOIS For Unilateral Vocal Fold ParalysisDokument8 Seiten2023 Apr - Pre Clinical Evaluation of APrevent VOIS For Unilateral Vocal Fold ParalysisemilylinNoch keine Bewertungen
- 2019 BatainehDokument10 Seiten2019 BatainehChristopher Cadete de FigueiredoNoch keine Bewertungen
- Adeno AnakDokument6 SeitenAdeno Anakokky_rahmatNoch keine Bewertungen
- Liu 2017Dokument7 SeitenLiu 2017jeff leeNoch keine Bewertungen
- Sup-1Dokument4 SeitenSup-1felaxis fNoch keine Bewertungen
- Cochlear-Implants Brochure 2Dokument2 SeitenCochlear-Implants Brochure 2roroNoch keine Bewertungen
- Signs and Symptoms of Temporomandibular Joint Disorders Related To The Degree of Mouth Opening and Hearing LossDokument9 SeitenSigns and Symptoms of Temporomandibular Joint Disorders Related To The Degree of Mouth Opening and Hearing LossFelipeSanzNoch keine Bewertungen
- 2012 Locatizacao ICDokument4 Seiten2012 Locatizacao ICEulalia JuanNoch keine Bewertungen
- OOOO Ricucci 2000Dokument6 SeitenOOOO Ricucci 2000karlaNoch keine Bewertungen
- Jurding Cochlea ImplantasiDokument53 SeitenJurding Cochlea ImplantasipuspitaNoch keine Bewertungen
- Recent Advancements in The Regeneration of Auditory Hair Cells and Hearing RestorationDokument16 SeitenRecent Advancements in The Regeneration of Auditory Hair Cells and Hearing RestorationRana Sabouni TabariNoch keine Bewertungen
- Bhutiani Et Al 2020 Assessment of Treatment Outcome of Presurgical Nasoalveolar Molding in Patients With Cleft Lip andDokument7 SeitenBhutiani Et Al 2020 Assessment of Treatment Outcome of Presurgical Nasoalveolar Molding in Patients With Cleft Lip andHenry Adhy SantosoNoch keine Bewertungen
- Jurnal 1 Titin SuhartinaDokument8 SeitenJurnal 1 Titin SuhartinaTitinNoch keine Bewertungen
- Vocal Fold Insuf Ficiency: Medialization Laryngoplasty Vs Calcium Hydroxylapatite Microspheres (Radiesse Voice)Dokument6 SeitenVocal Fold Insuf Ficiency: Medialization Laryngoplasty Vs Calcium Hydroxylapatite Microspheres (Radiesse Voice)Dr. Hilder HernandezNoch keine Bewertungen
- J Clinic Periodontology - 2020 - Jepsen - Vital Root Resection in Severely Furcation Involved Maxillary Molars OutcomesDokument10 SeitenJ Clinic Periodontology - 2020 - Jepsen - Vital Root Resection in Severely Furcation Involved Maxillary Molars OutcomesRosvin FernandezNoch keine Bewertungen
- Sun Et Al 2021 Comparison of Auricle Reconstruction With Expanded Flaps and Auricle Reconstruction With Non ExpandedDokument9 SeitenSun Et Al 2021 Comparison of Auricle Reconstruction With Expanded Flaps and Auricle Reconstruction With Non ExpandedMaico Rendón de la CruzNoch keine Bewertungen
- Tinnitus Heterogeneity on Auditory and Psychological CharacteristicsDokument4 SeitenTinnitus Heterogeneity on Auditory and Psychological CharacteristicsMateus NicacioNoch keine Bewertungen
- Arraño 2020Dokument7 SeitenArraño 2020Dome CárdenasNoch keine Bewertungen
- Chemical Engineer Skill SetDokument2 SeitenChemical Engineer Skill SetJunaid AhmadNoch keine Bewertungen
- Desoldering Tool: Designed For Lead FreeDokument2 SeitenDesoldering Tool: Designed For Lead FreeMarco Antonio Ortiz RomeroNoch keine Bewertungen
- The Poem of The Man God Vol 2 by Maria ValtortaDokument8 SeitenThe Poem of The Man God Vol 2 by Maria ValtortaOtieno SteveNoch keine Bewertungen
- Web Based Attendance Management SystemDokument19 SeitenWeb Based Attendance Management SystemAnonymous zenL7LNoch keine Bewertungen
- Wartsila O E W 50DF PG Product GuideDokument180 SeitenWartsila O E W 50DF PG Product GuideFábio Almeida100% (1)
- EMI and ACDokument14 SeitenEMI and ACbharathNoch keine Bewertungen
- Danfoss Saginomiya FQS - 1Dokument2 SeitenDanfoss Saginomiya FQS - 1istorletNoch keine Bewertungen
- Cyber Security and Reliability in A Digital CloudDokument95 SeitenCyber Security and Reliability in A Digital CloudBob GourleyNoch keine Bewertungen
- Hammer MillDokument4 SeitenHammer MillAnil Kumar KnNoch keine Bewertungen
- Microsoft Outlook QuestionDokument1 SeiteMicrosoft Outlook QuestionRipunjay MishraNoch keine Bewertungen
- Consultants New Rates GR Dated 09.05.2019Dokument11 SeitenConsultants New Rates GR Dated 09.05.2019Shakti SinghNoch keine Bewertungen
- GAC-12-VX-RMH-LAH-008 - Attachments - 1 To 7Dokument14 SeitenGAC-12-VX-RMH-LAH-008 - Attachments - 1 To 7Dipayan DasNoch keine Bewertungen
- DE12 Engine Injection Pump Replacement GuideDokument8 SeitenDE12 Engine Injection Pump Replacement GuidevarthotNoch keine Bewertungen
- F-Shaped Pattern For Reading Web ContentDokument3 SeitenF-Shaped Pattern For Reading Web Contentbortles1Noch keine Bewertungen
- Microsoft Dynamics ERP By: Nora Al-MadiDokument15 SeitenMicrosoft Dynamics ERP By: Nora Al-Madivijay_sr2009Noch keine Bewertungen
- HSM USB Serial Driver Release NotesDokument16 SeitenHSM USB Serial Driver Release NotesErnu AnatolieNoch keine Bewertungen
- Annual Report Nutek 2008 09Dokument92 SeitenAnnual Report Nutek 2008 09avneesh99Noch keine Bewertungen
- Zero Escape Virtues Last Reward PDFDokument33 SeitenZero Escape Virtues Last Reward PDFfcaicedo7239Noch keine Bewertungen
- HP TruCluster Server V5.1ADokument21 SeitenHP TruCluster Server V5.1AAlexandru BotnariNoch keine Bewertungen
- Midterm Exam Summary For Data Communications PDFDokument9 SeitenMidterm Exam Summary For Data Communications PDFKit Jason MonjeNoch keine Bewertungen
- Success and Failure Factors of BPRDokument29 SeitenSuccess and Failure Factors of BPRMohammad Hamid MahmoodNoch keine Bewertungen
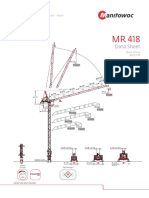
- MR418-FEM-Top Slewing Tower Cranes Imperial PDFDokument8 SeitenMR418-FEM-Top Slewing Tower Cranes Imperial PDFCompass equipmentNoch keine Bewertungen
- EM100 Training PDFDokument111 SeitenEM100 Training PDFAris Bodhi R0% (1)
- Gigabyte Sandy Bridge Overclocking GuideDokument27 SeitenGigabyte Sandy Bridge Overclocking GuideGIGABYTE UK100% (2)
- Conference Phone Peoplelink Quadro With Extension MicrophonesDokument3 SeitenConference Phone Peoplelink Quadro With Extension MicrophonessanjuktNoch keine Bewertungen
- SMPS Application NotesDokument4 SeitenSMPS Application Notesalguien1972Noch keine Bewertungen
- 410e Repair ExampleDokument6 Seiten410e Repair ExampleYurii Chinov71% (7)
- QCAI476 LfiltersDokument11 SeitenQCAI476 LfilterscivodulNoch keine Bewertungen
- QCL Certification Pvt. LTDDokument3 SeitenQCL Certification Pvt. LTDRamaKantDixitNoch keine Bewertungen