Das könnte Ihnen auch gefallen
- Surgery Shelf Notes 2021 PDFDokument43 SeitenSurgery Shelf Notes 2021 PDFBhandari SadikshyaNoch keine Bewertungen
- Pharmacology Quick Reference for Health Care ProvidersVon EverandPharmacology Quick Reference for Health Care ProvidersNoch keine Bewertungen
- Platelet Counting Fordirect Indirect MethodDokument30 SeitenPlatelet Counting Fordirect Indirect MethodShana Flame Haze100% (2)
- Nursing Health Assessment MnemonicsDokument20 SeitenNursing Health Assessment Mnemonicsmildred alidonNoch keine Bewertungen
- Drug Study FormatDokument2 SeitenDrug Study FormatEmilie CajaNoch keine Bewertungen
- NCP-Ineffective AirwayDokument5 SeitenNCP-Ineffective Airwayjava_biscocho1229Noch keine Bewertungen
- Spinal Cord Injury NCPDokument2 SeitenSpinal Cord Injury NCPEmmanuelRodriguez100% (1)
- Pharma Mod 11Dokument12 SeitenPharma Mod 11ANGELA SHANE AGUSTINNoch keine Bewertungen
- Prof BSP - Neurologic Paraneoplastic SyndromesDokument122 SeitenProf BSP - Neurologic Paraneoplastic SyndromesSavitha BasriNoch keine Bewertungen
- Anti EmeticsDokument29 SeitenAnti EmeticsBezawit TsigeNoch keine Bewertungen
- Drug Study - DigoxinDokument2 SeitenDrug Study - DigoxinKian Herrera50% (2)
- M.SC Yoga SyllabusDokument29 SeitenM.SC Yoga SyllabusSenthil KumarNoch keine Bewertungen
- A Development of Freudian Metapsychology For Schisophrenia Artaloytia2014Dokument26 SeitenA Development of Freudian Metapsychology For Schisophrenia Artaloytia2014Fredy TolentoNoch keine Bewertungen
- Drug AnalysisDokument49 SeitenDrug Analysisjomalaw6714Noch keine Bewertungen
- Jin Gui Yao Lue (Acupuncture)Dokument2 SeitenJin Gui Yao Lue (Acupuncture)Tim SchlankNoch keine Bewertungen
- Drug Study AsDokument3 SeitenDrug Study Askev mondaNoch keine Bewertungen
- Pharmacologic ClassDokument4 SeitenPharmacologic ClassBianca Nicole Gacad FernandezNoch keine Bewertungen
- AntiemeticsDokument25 SeitenAntiemeticsPridho GaziansyahNoch keine Bewertungen
- ANTIEMETIKDokument23 SeitenANTIEMETIKshabrinaNoch keine Bewertungen
- Clincal Practice Guidelines For ECT IJP-23Dokument26 SeitenClincal Practice Guidelines For ECT IJP-23JagadishaThirthalliNoch keine Bewertungen
- 1-Antiemetic DrugsDokument13 Seiten1-Antiemetic Drugsbwalyakangwa582Noch keine Bewertungen
- Psychiatric DrugDokument10 SeitenPsychiatric DrugKollebeng Pangda PasiwatNoch keine Bewertungen
- ER Drug StudyDokument4 SeitenER Drug StudyNecy Tessa C. AcostaNoch keine Bewertungen
- Bonilla Drug Study 2 20Dokument9 SeitenBonilla Drug Study 2 20YLA KATRINA BONILLANoch keine Bewertungen
- DepakoteDokument2 SeitenDepakotedana100% (1)
- Angiotensin-Converting Enzyme Inhibitors, Beta-Adrenergic Blockers: DecreasedDokument3 SeitenAngiotensin-Converting Enzyme Inhibitors, Beta-Adrenergic Blockers: DecreasedBianca Nicole Gacad FernandezNoch keine Bewertungen
- Anest Implication of PsikoaktifDokument5 SeitenAnest Implication of PsikoaktifjilieNoch keine Bewertungen
- Drug StudyDokument27 SeitenDrug StudyMariefer EsplagoNoch keine Bewertungen
- Antiemetic Drugs: PHR Sangita ShakyaDokument26 SeitenAntiemetic Drugs: PHR Sangita ShakyaCurex QANoch keine Bewertungen
- Anti-Emetic DrugsDokument10 SeitenAnti-Emetic DrugsLydia Alexandra LatumahinaNoch keine Bewertungen
- DRUGDokument6 SeitenDRUGjhoyorlyn22Noch keine Bewertungen
- Antiemitics & AntacidDokument22 SeitenAntiemitics & AntacidMohammad HayajnehNoch keine Bewertungen
- AntiemeticsDokument33 SeitenAntiemeticsSaiNoch keine Bewertungen
- Risperidone: Generic Name: ClassificationsDokument9 SeitenRisperidone: Generic Name: ClassificationsColeen Mae CamaristaNoch keine Bewertungen
- Guidelines For The Acute Assessment and Management of Amphetamine-Type Stimulant Intoxication and ToxicityDokument4 SeitenGuidelines For The Acute Assessment and Management of Amphetamine-Type Stimulant Intoxication and ToxicityTanani 102014007Noch keine Bewertungen
- Drug Induced VomitingDokument5 SeitenDrug Induced VomitingnimasNoch keine Bewertungen
- Standards of Laboratory Practice: Antiepileptic Drug MonitoringDokument11 SeitenStandards of Laboratory Practice: Antiepileptic Drug MonitoringDiegoAndrésYiZapataNoch keine Bewertungen
- Drug StudyDokument49 SeitenDrug StudyLexa Moreene Cu�adoNoch keine Bewertungen
- Psychotropic Substance Hallucinogens and Dissociatives - CompressedDokument39 SeitenPsychotropic Substance Hallucinogens and Dissociatives - CompressedshuyuichewNoch keine Bewertungen
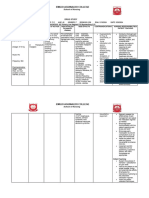
- Drug Name Classification Mechanism of Action Indications Contra Indications Side Effects Nursing ResponsibilitiesDokument5 SeitenDrug Name Classification Mechanism of Action Indications Contra Indications Side Effects Nursing ResponsibilitiesJessica FabroaNoch keine Bewertungen
- Drugs For Gastrointestinal Disorders 2023Dokument23 SeitenDrugs For Gastrointestinal Disorders 2023aguilarjanicaNoch keine Bewertungen
- Antimicrobial Regimen Selection (Quick AnswersL Pharmacy Book)Dokument16 SeitenAntimicrobial Regimen Selection (Quick AnswersL Pharmacy Book)Yasmin ElsobkyNoch keine Bewertungen
- Neuropathic Pain: Emerging TreatmentsDokument11 SeitenNeuropathic Pain: Emerging TreatmentsFarhatNoch keine Bewertungen
- Antipsychotic Drugs - Pharmacology - An Illustrated ReviewDokument5 SeitenAntipsychotic Drugs - Pharmacology - An Illustrated ReviewDragutin PetrićNoch keine Bewertungen
- Finals Activity 1 - Drug StudyDokument5 SeitenFinals Activity 1 - Drug StudyElly LazaroNoch keine Bewertungen
- Adrenergic Drugs: Pharmacological Department Medical School - UNPAD Ike HusenDokument33 SeitenAdrenergic Drugs: Pharmacological Department Medical School - UNPAD Ike HusenHendra EfendiNoch keine Bewertungen
- The Serotonin Syndrome: D. BijlDokument6 SeitenThe Serotonin Syndrome: D. BijlBianca CaterinalisendraNoch keine Bewertungen
- Emergency Presentations of MDDokument10 SeitenEmergency Presentations of MDGustavo PestanaNoch keine Bewertungen
- AkathisiaDokument4 SeitenAkathisiaRindayu Julianti NurmanNoch keine Bewertungen
- Pharmacology Module For FinalsDokument11 SeitenPharmacology Module For FinalsCarlo GaradoNoch keine Bewertungen
- Phle Module 4Dokument135 SeitenPhle Module 4Margaret RNoch keine Bewertungen
- YAWAADokument10 SeitenYAWAAZyrene CapulongNoch keine Bewertungen
- Acute Pain Management: Bruce Ferrell, MD Brandon Koretz, MDDokument5 SeitenAcute Pain Management: Bruce Ferrell, MD Brandon Koretz, MDJayagopi KadarasenNoch keine Bewertungen
- Citicoline Drug StudyDokument2 SeitenCiticoline Drug StudyJC LumayaNoch keine Bewertungen
- Anti Emetics, Prokinetic and Digestive DrugsDokument46 SeitenAnti Emetics, Prokinetic and Digestive DrugsCynthia KeruboNoch keine Bewertungen
- Polytechnic College of Davao Del Sur, Inc.: Drug StudyDokument2 SeitenPolytechnic College of Davao Del Sur, Inc.: Drug StudyDayanaj OngNoch keine Bewertungen
- Cerenia InjectableDokument2 SeitenCerenia InjectableRue BensonNoch keine Bewertungen
- UntitledDokument2 SeitenUntitledPRINCESS KOBAYASHINoch keine Bewertungen
- Apt Aka 2015Dokument3 SeitenApt Aka 2015dzakiyah nurul israNoch keine Bewertungen
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDokument1 SeiteAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Noch keine Bewertungen
- Drug-Induced Movement Disorders: TremorDokument6 SeitenDrug-Induced Movement Disorders: TremordentsavvyNoch keine Bewertungen
- Antidepressants, Antihistamines, General Anesthetics, MAO Inhibitors, OpioidsDokument3 SeitenAntidepressants, Antihistamines, General Anesthetics, MAO Inhibitors, Opioidskaycelyn jimenezNoch keine Bewertungen
- Antiemetic Drugs PDFDokument12 SeitenAntiemetic Drugs PDFDanisha Laila100% (2)
- PH - Karrar HaderDokument33 SeitenPH - Karrar HaderAdnan YassinNoch keine Bewertungen
- Adrenergic Agents: University of Negros Occidental-RecoletosDokument66 SeitenAdrenergic Agents: University of Negros Occidental-Recoletosmary grace trinidadNoch keine Bewertungen
- DrugsDokument8 SeitenDrugsJasmine J. FloresNoch keine Bewertungen
- DrUG STUDY PSYCHEDokument52 SeitenDrUG STUDY PSYCHELiza MPNoch keine Bewertungen
- NAUSEA AND VOMITING - ObatDokument8 SeitenNAUSEA AND VOMITING - ObatSri Ayu NingsihNoch keine Bewertungen
- Mental Health Proposal RevisedDokument7 SeitenMental Health Proposal Revisedapi-316749800Noch keine Bewertungen
- Exam Study Guide and Worksheet - Respiratory SystemDokument4 SeitenExam Study Guide and Worksheet - Respiratory SystemHailey PedenNoch keine Bewertungen
- Paediatric Consumer Health in IndiaDokument8 SeitenPaediatric Consumer Health in IndiaAkash GuruNoch keine Bewertungen
- IAEA Safety Standards: SSG-46Dokument340 SeitenIAEA Safety Standards: SSG-46Asiah HasanahNoch keine Bewertungen
- Electrotherapy: DR Ramaiah Choudhary PhysiotherapistDokument13 SeitenElectrotherapy: DR Ramaiah Choudhary Physiotherapistvenkata ramakrishnaiahNoch keine Bewertungen
- CompendiumDokument3 SeitenCompendiumKhuong LamNoch keine Bewertungen
- Sinusoidal CurrentDokument16 SeitenSinusoidal CurrentHareem Fatima100% (1)
- Clough K Oncoplasty BJSDokument7 SeitenClough K Oncoplasty BJSkomlanihou_890233161Noch keine Bewertungen
- Presented By: Christopher H. Wise, PT, DPT, MS, OCS, FAAOMPT, MTC, ATCDokument1 SeitePresented By: Christopher H. Wise, PT, DPT, MS, OCS, FAAOMPT, MTC, ATCemilNoch keine Bewertungen
- Risk Factors For Postoperative Nausea and VomitingDokument21 SeitenRisk Factors For Postoperative Nausea and VomitingmusafirlautNoch keine Bewertungen
- Conquering Interview AnxietyDokument4 SeitenConquering Interview AnxietySai Pavan KumarNoch keine Bewertungen
- Objectives: Therapeutic DietDokument17 SeitenObjectives: Therapeutic DietKBDNoch keine Bewertungen
- Stages of ReadingDokument12 SeitenStages of ReadingRolando Vilches GonzalezNoch keine Bewertungen
- Microfracture and Microfracture PlusDokument7 SeitenMicrofracture and Microfracture PlusdrjorgewtorresNoch keine Bewertungen
- Diabetic Retinopathy in PregnancyDokument109 SeitenDiabetic Retinopathy in PregnancyrayshahNoch keine Bewertungen
- Case ReportDokument50 SeitenCase ReportTajul AnshorNoch keine Bewertungen
- Mitral Valve ProlapseDokument4 SeitenMitral Valve Prolapseapi-306423962Noch keine Bewertungen
- Hypertensive Disorders of Pregnancy Teaching PlanDokument5 SeitenHypertensive Disorders of Pregnancy Teaching PlanMary Grace Belmonte100% (1)
- Draeger Evita V800 GE R860Dokument2 SeitenDraeger Evita V800 GE R860Billy IrawanNoch keine Bewertungen
- Program and Proceedings - 4th Caribbean Biomedical Research Days CBRD-2017, Jan 16-18, 2017, Rodney Bay, St. LuciaDokument18 SeitenProgram and Proceedings - 4th Caribbean Biomedical Research Days CBRD-2017, Jan 16-18, 2017, Rodney Bay, St. LuciaISBS_SocietyNoch keine Bewertungen
- Table AlkesDokument14 SeitenTable Alkesintan purnama sariNoch keine Bewertungen
- GBV Monthly Work PlanDokument20 SeitenGBV Monthly Work Planrachaelnamz19Noch keine Bewertungen