Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 2013 BCF Stallion Auction CatalogDokument31 Seiten2013 BCF Stallion Auction Catalogapi-85716849Noch keine Bewertungen
- Butterflies and MothsDokument3 SeitenButterflies and MothsZoora SavioNoch keine Bewertungen
- Farmer, Philip Jose - The Stone God AwakensDokument136 SeitenFarmer, Philip Jose - The Stone God AwakenswothboraNoch keine Bewertungen
- Spinal Cord - Gross AnatomyDokument2 SeitenSpinal Cord - Gross AnatomyshreyasNoch keine Bewertungen
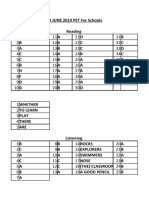
- Keys For Pet Exam PackDokument34 SeitenKeys For Pet Exam PackEleftheria AggeleaNoch keine Bewertungen
- Sealing of The Five Senses - Opening of The Crystal Room PDFDokument47 SeitenSealing of The Five Senses - Opening of The Crystal Room PDFAlexandra Ioana NiculescuNoch keine Bewertungen
- Descriptive Text About Place: DolphinsDokument2 SeitenDescriptive Text About Place: DolphinsIsmiweningNoch keine Bewertungen
- My First English Exam PDFDokument86 SeitenMy First English Exam PDFCiprian PetcuNoch keine Bewertungen
- Portuguese Lamnguage Part 2Dokument20 SeitenPortuguese Lamnguage Part 2nunoNoch keine Bewertungen
- Bald Eagle PDFDokument4 SeitenBald Eagle PDFangeunkacangNoch keine Bewertungen
- مقدمة علم التشريحDokument64 Seitenمقدمة علم التشريحsayfmohammed719Noch keine Bewertungen
- Cells JeopardyDokument55 SeitenCells Jeopardyapi-308745623Noch keine Bewertungen
- Fritz NotesDokument4 SeitenFritz NotesSnehasish Bar50% (2)
- Squid Game CharactersDokument20 SeitenSquid Game CharactersJose Ramon Batiller100% (1)
- Asian Hornet (Vespa Velutina) Response PlanDokument11 SeitenAsian Hornet (Vespa Velutina) Response PlanPeter Anthony MartinsNoch keine Bewertungen
- Gnomo Sombrero de Arbol - PDF Versión 1Dokument26 SeitenGnomo Sombrero de Arbol - PDF Versión 1Talla Arriazu ElgueaNoch keine Bewertungen
- Virus ZikaDokument2 SeitenVirus Zikainta hestyaNoch keine Bewertungen
- Animal ClassificationDokument4 SeitenAnimal ClassificationKiyotaka BautistaNoch keine Bewertungen
- Get To Know Detachable Clipper Blades - Ivan Zoot - Clipper Guy Says...Dokument8 SeitenGet To Know Detachable Clipper Blades - Ivan Zoot - Clipper Guy Says...Ivan Zoot100% (4)
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Dokument8 SeitenSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- Kitchen TerminologyDokument28 SeitenKitchen TerminologyMariam SalongaNoch keine Bewertungen
- S 123 Sept 17060917Dokument41 SeitenS 123 Sept 17060917rockmanqhNoch keine Bewertungen
- Francisco FrondaDokument2 SeitenFrancisco FrondaAva BarramedaNoch keine Bewertungen
- Pathophysiology Exam 4 - ReviewDokument18 SeitenPathophysiology Exam 4 - ReviewWaqas GillNoch keine Bewertungen
- MiniVetGuide Infographics I Final 16092019 PrintfriendlyDokument1 SeiteMiniVetGuide Infographics I Final 16092019 PrintfriendlyEnalDgm100% (1)
- Tehnik - Tehnik MenjahitDokument6 SeitenTehnik - Tehnik MenjahitBang mantoNoch keine Bewertungen
- Class 11 Biology NCERT Textbook Chapter 1 The Living WorldDokument20 SeitenClass 11 Biology NCERT Textbook Chapter 1 The Living WorldROHAN SHARMANoch keine Bewertungen
- Nature's Pathways Jan 2012 Issue - Northeast WI EditionDokument108 SeitenNature's Pathways Jan 2012 Issue - Northeast WI EditionNature's PathwaysNoch keine Bewertungen
- Bikalpa 19Dokument28 SeitenBikalpa 19Ebang BikalpaNoch keine Bewertungen
- First Page PDFDokument1 SeiteFirst Page PDFvarshasharma05Noch keine Bewertungen