Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- NCM 103 (LEC) : Electrocardiogram (ECG) ElectrocardiogramDokument10 SeitenNCM 103 (LEC) : Electrocardiogram (ECG) ElectrocardiogramJohn Protacio50% (2)
- Seizure-Case StudyDokument6 SeitenSeizure-Case StudyELaine ELena TiongsonNoch keine Bewertungen
- Acute Coronary Syndrome - AMBOSSDokument31 SeitenAcute Coronary Syndrome - AMBOSSSarah Ronquillo100% (1)
- Visceral OMT: AAO Convocation March 2018 Kenneth Lossing DODokument59 SeitenVisceral OMT: AAO Convocation March 2018 Kenneth Lossing DODiana SchlittlerNoch keine Bewertungen
- Tetanus ProtocolDokument6 SeitenTetanus ProtocolRebecca BlackburnNoch keine Bewertungen
- Hypertrophic CardiomyopathyDokument10 SeitenHypertrophic CardiomyopathySam SonNoch keine Bewertungen
- 2 5210764081396449976 PDFDokument1 Seite2 5210764081396449976 PDFranggaNoch keine Bewertungen
- Pathogenesis of Dystonia: Is It of Cerebellar or Basal Ganglia Origin?Dokument5 SeitenPathogenesis of Dystonia: Is It of Cerebellar or Basal Ganglia Origin?Ana Isabel CastañedaNoch keine Bewertungen
- STR 53 1540Dokument10 SeitenSTR 53 1540ranggaNoch keine Bewertungen
- 2 5210708435800163509 PDFDokument25 Seiten2 5210708435800163509 PDFranggaNoch keine Bewertungen
- PENdukung TetanusDokument29 SeitenPENdukung TetanusranggaNoch keine Bewertungen
- RCT Tetanus TX With Tetanus Antiglobulin PDFDokument4 SeitenRCT Tetanus TX With Tetanus Antiglobulin PDFranggaNoch keine Bewertungen
- Long-Term Pulmonary FunctionDokument12 SeitenLong-Term Pulmonary FunctionranggaNoch keine Bewertungen
- Alberta TetanusDokument7 SeitenAlberta TetanusranggaNoch keine Bewertungen
- Peniciline Vs MetroDokument3 SeitenPeniciline Vs MetroranggaNoch keine Bewertungen
- Alberta TetanusDokument7 SeitenAlberta TetanusranggaNoch keine Bewertungen
- TetanusDokument12 SeitenTetanustinkerbell03Noch keine Bewertungen
- Differentialdiagnosisofdiscedema2 170510195516Dokument69 SeitenDifferentialdiagnosisofdiscedema2 170510195516ranggaNoch keine Bewertungen
- Menongioma PPT Slidshare PDFDokument75 SeitenMenongioma PPT Slidshare PDFranggaNoch keine Bewertungen
- J Natl Compr Canc Netw 2017 Nabors 1331 45Dokument15 SeitenJ Natl Compr Canc Netw 2017 Nabors 1331 45ranggaNoch keine Bewertungen
- 10 1053@j Ro 2017 11 005 PDFDokument50 Seiten10 1053@j Ro 2017 11 005 PDFranggaNoch keine Bewertungen
- Teleconference3 230517 Post Dengue Myelitis eDokument1 SeiteTeleconference3 230517 Post Dengue Myelitis eranggaNoch keine Bewertungen
- Tens For LBPDokument11 SeitenTens For LBPranggaNoch keine Bewertungen
- Tinnitus Ringing in The EarsDokument11 SeitenTinnitus Ringing in The EarsWibi GunawanNoch keine Bewertungen
- How Alcohol Changes Your BodyDokument14 SeitenHow Alcohol Changes Your BodyyuliNoch keine Bewertungen
- Schools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasDokument2 SeitenSchools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasSharna Flynn SolonNoch keine Bewertungen
- Respiratory SystemDokument13 SeitenRespiratory Systemapi-270700888Noch keine Bewertungen
- NICaS Study Review 2Dokument158 SeitenNICaS Study Review 2Dzikrul Haq KarimullahNoch keine Bewertungen
- A Mathematical Model of The Human Respiratory System: W.F. Fincham and F.T. TehraniDokument9 SeitenA Mathematical Model of The Human Respiratory System: W.F. Fincham and F.T. TehraniDayana VieiraNoch keine Bewertungen
- So April 2023Dokument36 SeitenSo April 2023elisantagrace brawijayalaboratoryNoch keine Bewertungen
- Pernicious Anemia: Nursing Care of Patient WithDokument16 SeitenPernicious Anemia: Nursing Care of Patient WithMuhammad Jefri LukmanNoch keine Bewertungen
- Ventricular FibrillationDokument6 SeitenVentricular FibrillationclubsanatateNoch keine Bewertungen
- Owl NecropsyDokument3 SeitenOwl Necropsykezia_stephanie_1Noch keine Bewertungen
- Science - 1.3 Stimuli and Responses in PlantsDokument10 SeitenScience - 1.3 Stimuli and Responses in PlantsJierui NgNoch keine Bewertungen
- Antiarrhythmic Drugs - AMBOSS TWO PDFDokument6 SeitenAntiarrhythmic Drugs - AMBOSS TWO PDFRuva Oscass JimmyNoch keine Bewertungen
- Manoj SirDokument27 SeitenManoj SirANKURNoch keine Bewertungen
- L7 Muscles 14 15 STDokument78 SeitenL7 Muscles 14 15 STLenny MerdhaNoch keine Bewertungen
- Microlife BP 3AC1 1 ManualDokument80 SeitenMicrolife BP 3AC1 1 ManualJulian GarcíaNoch keine Bewertungen
- Reference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Dokument3 SeitenReference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Kris Marie DelaCruz DomingoNoch keine Bewertungen
- Glycolysis: Glycolysis (From Glycose, An Older TermDokument3 SeitenGlycolysis: Glycolysis (From Glycose, An Older TermProff AhengNoch keine Bewertungen
- Similarities Between Cellular Respiration and PhotosynthesisDokument4 SeitenSimilarities Between Cellular Respiration and PhotosynthesisShelline OyooNoch keine Bewertungen
- CN 118 - Assessment (Reviewer)Dokument5 SeitenCN 118 - Assessment (Reviewer)Camille SanguyoNoch keine Bewertungen
- Garcia - Assignment1 - Ipe 402aDokument2 SeitenGarcia - Assignment1 - Ipe 402aAron GarciaNoch keine Bewertungen
- Role of Pathya Apathya in VranaDokument6 SeitenRole of Pathya Apathya in VranaEditor IJTSRDNoch keine Bewertungen
- Cardiorespiratory Arrest (FS)Dokument88 SeitenCardiorespiratory Arrest (FS)haerul ikhsanNoch keine Bewertungen
- Human HeartDokument7 SeitenHuman HeartAsher Eby VargeeseNoch keine Bewertungen
- Dissection Lab PDFDokument6 SeitenDissection Lab PDFEunnie ChongNoch keine Bewertungen
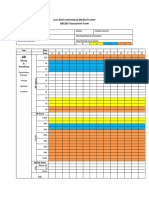
- Jose Rizal University & Medical Center: ABCDEF Assessment FormDokument3 SeitenJose Rizal University & Medical Center: ABCDEF Assessment FormMichael SarmientoNoch keine Bewertungen
- Sensorium.: NiirDokument6 SeitenSensorium.: NiirSundar RajanNoch keine Bewertungen