Das könnte Ihnen auch gefallen
- List of All Run Commands For WindowsDokument10 SeitenList of All Run Commands For Windowsdixityog100% (1)
- Commentary On The Book of NahumDokument9 SeitenCommentary On The Book of NahumRev Dr Jeffry Camm JP, MIEPR, MISOPNoch keine Bewertungen
- Onechanbara - Bikini Samurai Squad Game GuideDokument83 SeitenOnechanbara - Bikini Samurai Squad Game GuideStefan RoscaNoch keine Bewertungen
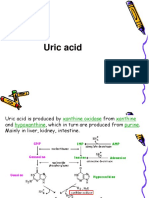
- Uric AcidDokument30 SeitenUric AcidKesavanVeeraNoch keine Bewertungen
- Types of Media and Media ConvergenceDokument70 SeitenTypes of Media and Media ConvergenceYsmile De LaraNoch keine Bewertungen
- Kidney Stones - A ReviewDokument18 SeitenKidney Stones - A ReviewViall Ivenka100% (1)
- Once Upon A Timein AmericaDokument335 SeitenOnce Upon A Timein Americaqwerty-keysNoch keine Bewertungen
- The Magical Diaries of Ethel ArcherDokument7 SeitenThe Magical Diaries of Ethel Archerleeghancock100% (1)
- Case Study of AmoebiasisDokument16 SeitenCase Study of AmoebiasisGlorielle ElvambuenaNoch keine Bewertungen
- Of Gods, Glyphs and KingsDokument24 SeitenOf Gods, Glyphs and KingsBraulioNoch keine Bewertungen
- China Email ListDokument3 SeitenChina Email ListRosie Brown40% (5)
- Bus Bar Arrangement of SubstationDokument17 SeitenBus Bar Arrangement of SubstationBbimafidon_248613673Noch keine Bewertungen
- WWW Creativebloq Com Infographic Tools 2131971Dokument20 SeitenWWW Creativebloq Com Infographic Tools 2131971Martin_Arrieta_GNoch keine Bewertungen
- Urinary Stones: Medical and Surgical ManagementVon EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNoch keine Bewertungen
- Treatment of Asymptomatic Hyperuricemia in Chronic Kidney DiseaseDokument4 SeitenTreatment of Asymptomatic Hyperuricemia in Chronic Kidney DiseaseRonald Ariyanto WiradirnataNoch keine Bewertungen
- Renal Calculi AComprehensive ReviewDokument6 SeitenRenal Calculi AComprehensive ReviewPankaj RathvaNoch keine Bewertungen
- Epidemiology Pathophysiology and Management of Uric - 2017 - Journal of AdvanDokument15 SeitenEpidemiology Pathophysiology and Management of Uric - 2017 - Journal of AdvanMilind J.Noch keine Bewertungen
- Optimum Nutrition For Kidney Stone DiseaseDokument10 SeitenOptimum Nutrition For Kidney Stone DiseaseAlonso MedinaNoch keine Bewertungen
- Medical Therapy For Nephrolithiasis: State of The Art: SciencedirectDokument13 SeitenMedical Therapy For Nephrolithiasis: State of The Art: SciencedirectReffada YodhyasenaNoch keine Bewertungen
- The Management of UrolithiasisDokument9 SeitenThe Management of UrolithiasiselhaanNoch keine Bewertungen
- Preventive Kidney Stones: Continue Medical Education: Review ArticleDokument6 SeitenPreventive Kidney Stones: Continue Medical Education: Review ArticleLusianaTasyaNoch keine Bewertungen
- Tju 46 Supplement1 s92Dokument12 SeitenTju 46 Supplement1 s92Rohma YuliaNoch keine Bewertungen
- Ipi 522009Dokument5 SeitenIpi 522009Felia maiza ardilaNoch keine Bewertungen
- Uric AcidDokument6 SeitenUric Acidmonday125100% (1)
- Core Curriculum NefrolitiasisDokument13 SeitenCore Curriculum NefrolitiasisOscar MoralesNoch keine Bewertungen
- Lifestyle Recommendations To Reduce The Risk of Kidney StonesDokument8 SeitenLifestyle Recommendations To Reduce The Risk of Kidney Stonesjsali9210Noch keine Bewertungen
- Mjiem 1000120 PDFDokument6 SeitenMjiem 1000120 PDFwandaNoch keine Bewertungen
- 10.1177 1756287210369121 PDFDokument7 Seiten10.1177 1756287210369121 PDFasfwegereNoch keine Bewertungen
- Correlation of Gallstone Disease With Iron Deficiency AnemiaDokument5 SeitenCorrelation of Gallstone Disease With Iron Deficiency AnemiaMudassar SattarNoch keine Bewertungen
- Prevalence and Risk Factors of Kidney Stone-ArticleDokument6 SeitenPrevalence and Risk Factors of Kidney Stone-ArticleReesky Nanda Rockn'rollNoch keine Bewertungen
- Kidney Stones: BMJ (Online) July 2004Dokument6 SeitenKidney Stones: BMJ (Online) July 2004Lina LopezNoch keine Bewertungen
- Urine ChemistryDokument11 SeitenUrine ChemistryPedia TricNoch keine Bewertungen
- Current Concepts of And: Hyperuricemia GoutDokument13 SeitenCurrent Concepts of And: Hyperuricemia GoutAnonymous h0XxWy8SNoch keine Bewertungen
- 10 2215@CJN 10330818Dokument11 Seiten10 2215@CJN 10330818paulina naranjoNoch keine Bewertungen
- NEFOLITIASISDokument10 SeitenNEFOLITIASISjim manuel dominguez rosalesNoch keine Bewertungen
- Patofisiologi Kidney StonesDokument8 SeitenPatofisiologi Kidney StonespipitNoch keine Bewertungen
- Cejph - Cjp-Faktor Penyebab UrolithiasisDokument6 SeitenCejph - Cjp-Faktor Penyebab UrolithiasisCDKadrianNoch keine Bewertungen
- Predictive Value of Kidney Stone Composition in The Detection of Metabolic AbnormalitiesDokument7 SeitenPredictive Value of Kidney Stone Composition in The Detection of Metabolic Abnormalitiesjarivera1300Noch keine Bewertungen
- Pathophysiology-Based Treatment of UrolithiasisDokument7 SeitenPathophysiology-Based Treatment of UrolithiasisLea Bali Ulina SinurayaNoch keine Bewertungen
- Biomarkers in UrolithiasisselloDokument11 SeitenBiomarkers in Urolithiasisselloregigaby02Noch keine Bewertungen
- Renal Stones A Clinical Review PDFDokument6 SeitenRenal Stones A Clinical Review PDFNurholis MajidNoch keine Bewertungen
- Pathophysiology of Nephrolithiasis PDFDokument9 SeitenPathophysiology of Nephrolithiasis PDFLayuganlovelyNoch keine Bewertungen
- Nephrolithiasis: Treatment, Causes, and PreventionDokument9 SeitenNephrolithiasis: Treatment, Causes, and PreventionMaxi SpositoNoch keine Bewertungen
- English UrolithiasisDokument7 SeitenEnglish UrolithiasisNurintan PermataNoch keine Bewertungen
- Pharmaceutical Sciences: Urinary Sodium and Potassium Discharge and Danger of Hypertension in Pakistani PopulationDokument4 SeitenPharmaceutical Sciences: Urinary Sodium and Potassium Discharge and Danger of Hypertension in Pakistani PopulationiajpsNoch keine Bewertungen
- Associations Between BMI, Serum Uric Acid, Serum Glucose, and Blood Pressure With Urinary Tract Stone OpacityDokument10 SeitenAssociations Between BMI, Serum Uric Acid, Serum Glucose, and Blood Pressure With Urinary Tract Stone OpacityIcutNoch keine Bewertungen
- Medical Management of Renal Stone: Review ArticleDokument4 SeitenMedical Management of Renal Stone: Review ArticlenaveenNoch keine Bewertungen
- Renal Stones in Children: Evaluation and Medical Management: Inoka V G PereraDokument8 SeitenRenal Stones in Children: Evaluation and Medical Management: Inoka V G Pererakrishnadoctor1Noch keine Bewertungen
- Primary Care Medicine: TopisDokument4 SeitenPrimary Care Medicine: TopisCarineNoch keine Bewertungen
- Enal Alculi: Renal Colic in Syllabus For Related D/D Type of Pain, Refer Notes Abdominal Pain. Sent On 7th August 2020Dokument8 SeitenEnal Alculi: Renal Colic in Syllabus For Related D/D Type of Pain, Refer Notes Abdominal Pain. Sent On 7th August 2020Viswa GiriNoch keine Bewertungen
- Bacteriological Evaluation of Bladder Calculi: A Study: Original Research ArticleDokument4 SeitenBacteriological Evaluation of Bladder Calculi: A Study: Original Research ArticleivanNoch keine Bewertungen
- Na CVDJHH2018Dokument10 SeitenNa CVDJHH2018Itsme AyNoch keine Bewertungen
- PatofisiologyDokument13 SeitenPatofisiologyarinNoch keine Bewertungen
- Answer Rationale: 2021 Long Quiz 1Dokument15 SeitenAnswer Rationale: 2021 Long Quiz 1Rix tanNoch keine Bewertungen
- Nutrients 13 04117 v2Dokument10 SeitenNutrients 13 04117 v2xavinwonderlandNoch keine Bewertungen
- Uric Acid in Chronic Kidney Disease: CA Murakami, SM SozioDokument6 SeitenUric Acid in Chronic Kidney Disease: CA Murakami, SM SozioHanny Friska YudistyawanNoch keine Bewertungen
- Nephrolithiasis in ChildrenDokument11 SeitenNephrolithiasis in Childrendiah_budiarti_1Noch keine Bewertungen
- SMJ - V2-3 - Lawrence Management of UrolithiasisDokument3 SeitenSMJ - V2-3 - Lawrence Management of Urolithiasishaulasitafadhilah1010711096Noch keine Bewertungen
- 07 Flannigan 2014 Nat Rev Urol Struvite StonesDokument10 Seiten07 Flannigan 2014 Nat Rev Urol Struvite StonesFranz CoriNoch keine Bewertungen
- Consumo Diario de Calcio y Oxalacetato en Humanos 2Dokument5 SeitenConsumo Diario de Calcio y Oxalacetato en Humanos 2Brain LongwoodNoch keine Bewertungen
- Validation of A Novel Diagnostic Test For Assessing The Risk of Urinary Uric ACID CRYSTALLIZACIONDokument6 SeitenValidation of A Novel Diagnostic Test For Assessing The Risk of Urinary Uric ACID CRYSTALLIZACIONMARIANNE CASTILLO ESCOBARNoch keine Bewertungen
- Kidney Stones Epidemiology 310107Dokument5 SeitenKidney Stones Epidemiology 310107veve1234Noch keine Bewertungen
- Asymptomatic Hyperuricemia and Chronic Kidney Disease - 2017 - Journal of AdvaDokument6 SeitenAsymptomatic Hyperuricemia and Chronic Kidney Disease - 2017 - Journal of AdvaMilind J.Noch keine Bewertungen
- Utility of Homoeopathic Medicines in Management of NephrolithiasisDokument7 SeitenUtility of Homoeopathic Medicines in Management of NephrolithiasisEditor IJTSRDNoch keine Bewertungen
- Review Article Renal Stone Disease: Causes, Evaluation and Medical TreatmentDokument9 SeitenReview Article Renal Stone Disease: Causes, Evaluation and Medical TreatmentZulfikar BasriNoch keine Bewertungen
- 2020 Metabolic Risk FactorsDokument6 Seiten2020 Metabolic Risk FactorsAngela LópezNoch keine Bewertungen
- Nutritional Management of Kidney Stones (Nephrolithiasis) : Clinical Nutrition Research July 2015Dokument17 SeitenNutritional Management of Kidney Stones (Nephrolithiasis) : Clinical Nutrition Research July 2015Mạnh LươngNoch keine Bewertungen
- Kidney and Ureteral StonesDokument12 SeitenKidney and Ureteral StonescubirojasNoch keine Bewertungen
- Understanding Epidemiology and Etiologic Factors of Urolithiasis: An OverviewDokument6 SeitenUnderstanding Epidemiology and Etiologic Factors of Urolithiasis: An OverviewandrilulusanterbaikNoch keine Bewertungen
- Nephrolithiasis: Grade A ReferencesDokument8 SeitenNephrolithiasis: Grade A ReferencesEngin AltınkayaNoch keine Bewertungen
- Gender Differences in Problematic Alcohol Consumption in University ProfessorsDokument11 SeitenGender Differences in Problematic Alcohol Consumption in University ProfessorssyifaNoch keine Bewertungen
- Evaluation of Alcoholic Consumption On Serum Uric Acid, Urea, and Creatinine LevelsDokument3 SeitenEvaluation of Alcoholic Consumption On Serum Uric Acid, Urea, and Creatinine LevelssyifaNoch keine Bewertungen
- Perbandingan Kadar Kreatinin Dan Asam Urat Pada Serum Dan Urin Penderita Hipertensi Dan NormotensiDokument9 SeitenPerbandingan Kadar Kreatinin Dan Asam Urat Pada Serum Dan Urin Penderita Hipertensi Dan NormotensisyifaNoch keine Bewertungen
- The Relation of Moderate Alcohol Consumption To Hyperuricemia in A Rural General PopulationDokument11 SeitenThe Relation of Moderate Alcohol Consumption To Hyperuricemia in A Rural General PopulationsyifaNoch keine Bewertungen
- International Research Journal of PharmacyDokument4 SeitenInternational Research Journal of PharmacysyifaNoch keine Bewertungen
- Correspondence: Alcohol Intake, Serum Uric Acid Concentrations, and Risk of GoutDokument2 SeitenCorrespondence: Alcohol Intake, Serum Uric Acid Concentrations, and Risk of GoutsyifaNoch keine Bewertungen
- Preventive MedicineDokument6 SeitenPreventive MedicinesyifaNoch keine Bewertungen
- Relationship of Serum Uric Acid Level With Non-Alcoholic Fatty Liver Disease and Its in Ammation Progression in Non-Obese AdultsDokument9 SeitenRelationship of Serum Uric Acid Level With Non-Alcoholic Fatty Liver Disease and Its in Ammation Progression in Non-Obese AdultssyifaNoch keine Bewertungen
- Relationship Between Dietary Beef, Fat, and Pork and Alcoholic CirrhosisDokument9 SeitenRelationship Between Dietary Beef, Fat, and Pork and Alcoholic CirrhosissyifaNoch keine Bewertungen
- Serum Uric Acid In: HypertensiveDokument6 SeitenSerum Uric Acid In: HypertensivesyifaNoch keine Bewertungen
- Inverse Association Between Coffee Drinking and Serum Uric Acid Concentrations in Middle-Aged Japanese MalesDokument6 SeitenInverse Association Between Coffee Drinking and Serum Uric Acid Concentrations in Middle-Aged Japanese MalessyifaNoch keine Bewertungen
- Alcohol Consumption in Oliver Twist: Literature As Prevention of AlcoholismDokument6 SeitenAlcohol Consumption in Oliver Twist: Literature As Prevention of AlcoholismsyifaNoch keine Bewertungen
- Ijerph 12 02411 PDFDokument26 SeitenIjerph 12 02411 PDFsyifaNoch keine Bewertungen
- Ijerph 07 04023Dokument14 SeitenIjerph 07 04023syifaNoch keine Bewertungen
- The Association Between Alcohol Consumption and - Cell Function and Insulin Sensitivity in Korean PopulationDokument11 SeitenThe Association Between Alcohol Consumption and - Cell Function and Insulin Sensitivity in Korean PopulationsyifaNoch keine Bewertungen
- Nitte University Journal June 2012-18-23Dokument11 SeitenNitte University Journal June 2012-18-23syifaNoch keine Bewertungen
- Nutrients: Association Between Alcohol Consumption, Folate Intake, and Risk of Pancreatic Cancer: A Case-Control StudyDokument9 SeitenNutrients: Association Between Alcohol Consumption, Folate Intake, and Risk of Pancreatic Cancer: A Case-Control StudysyifaNoch keine Bewertungen
- A Multilevel Study of Students in Vietnam: Drinking Motives and Drinking Context As Predictors of Alcohol ConsumptionDokument13 SeitenA Multilevel Study of Students in Vietnam: Drinking Motives and Drinking Context As Predictors of Alcohol ConsumptionsyifaNoch keine Bewertungen
- SSP 861603 - EN - Tire Pressure Monitoring SystemsDokument42 SeitenSSP 861603 - EN - Tire Pressure Monitoring Systemsa.diedrichsNoch keine Bewertungen
- Motivation MBADokument31 SeitenMotivation MBAAkshitaNoch keine Bewertungen
- Allama Iqbal Open University, Islamabad: (Secondary Teacher Education Department) WarningDokument2 SeitenAllama Iqbal Open University, Islamabad: (Secondary Teacher Education Department) WarningAiNa KhanNoch keine Bewertungen
- Engineering Discourse Communities RMDokument4 SeitenEngineering Discourse Communities RMapi-336463296Noch keine Bewertungen
- Reflection PseudoscienceDokument3 SeitenReflection PseudoscienceSuganthi RamasamyNoch keine Bewertungen
- Theological Differences Between Christianity and IslamDokument18 SeitenTheological Differences Between Christianity and IslamMencari KhadijahNoch keine Bewertungen
- 1.4 Creating Graphic OrganizerDokument1 Seite1.4 Creating Graphic OrganizerTrixie Roselle Y. MesiasNoch keine Bewertungen
- Lescture OPACDokument5 SeitenLescture OPACAgulto, Ivan R.Noch keine Bewertungen
- ReflectionDokument2 SeitenReflectionBảo HàNoch keine Bewertungen
- Essentials of Materials Science and Engineering Si Edition 3rd Edition Askeland Solutions ManualDokument11 SeitenEssentials of Materials Science and Engineering Si Edition 3rd Edition Askeland Solutions Manualjeffreyhayesagoisypdfm100% (13)
- Celebrations Around The WorldDokument3 SeitenCelebrations Around The WorldpaolaNoch keine Bewertungen
- Job Board Week WhituDokument5 SeitenJob Board Week WhituAnonymous MZh1KUUXNoch keine Bewertungen
- Implementasi Fault Management (Manajemen Kesalahan) Pada Network Management System (NMS) Berbasis SNMPDokument11 SeitenImplementasi Fault Management (Manajemen Kesalahan) Pada Network Management System (NMS) Berbasis SNMPIwoncl AsranNoch keine Bewertungen
- Ratio & Proportion Part 1Dokument5 SeitenRatio & Proportion Part 1P Singh KarkiNoch keine Bewertungen
- 850 Elective English QPDokument3 Seiten850 Elective English QPRudra SahaNoch keine Bewertungen
- Sticker BookDokument66 SeitenSticker BookIvan SutlovicNoch keine Bewertungen
- Crim 2 Module 2 Atty A.D.G.Dokument7 SeitenCrim 2 Module 2 Atty A.D.G.Badens DgNoch keine Bewertungen
- La Lit Review-Jennifer Draper-2-2Dokument9 SeitenLa Lit Review-Jennifer Draper-2-2api-653567856Noch keine Bewertungen
- Police Forces and The Administration of Justice in Tanzania.Dokument6 SeitenPolice Forces and The Administration of Justice in Tanzania.Praygod Manase100% (2)