Das könnte Ihnen auch gefallen
- AAP Developmental and Behavioral Pediatrics 2nd EditionDokument693 SeitenAAP Developmental and Behavioral Pediatrics 2nd Editionrina100% (13)
- Apple BenifitsDokument8 SeitenApple Benifitsnara4allNoch keine Bewertungen
- Antibiotic Prophylaxis in DentistryDokument9 SeitenAntibiotic Prophylaxis in DentistryLiana OpriţăNoch keine Bewertungen
- Dental Implants Are Contraindicated In...Dokument5 SeitenDental Implants Are Contraindicated In...Lia DietrichNoch keine Bewertungen
- Ampalaya Chips With Sweet DipDokument31 SeitenAmpalaya Chips With Sweet DipJayson San Juan86% (7)
- Fading Rainbow - Abm Sycipgroup 1 1Dokument14 SeitenFading Rainbow - Abm Sycipgroup 1 1Kate ParanaNoch keine Bewertungen
- Interpretation of OpgDokument6 SeitenInterpretation of Opgjawaad29375% (8)
- Diagnosis of Dental CariesDokument35 SeitenDiagnosis of Dental CariesKanika MalikNoch keine Bewertungen
- Invasive Ductal CarcinomaDokument51 SeitenInvasive Ductal CarcinomaGiselle Eclarino100% (2)
- Basics of Endodontics GuideDokument26 SeitenBasics of Endodontics GuideAreebaKhalidNoch keine Bewertungen
- 8 - Resin BondedDokument14 Seiten8 - Resin BondedÃmøĺã Hûśśiêñ100% (1)
- CHAPTER 13. Interdisciplinary ConsiderationsDokument13 SeitenCHAPTER 13. Interdisciplinary ConsiderationsAlina AnechiteiNoch keine Bewertungen
- Soumya S Jeena Profile BookDokument53 SeitenSoumya S Jeena Profile BooksoumyaNoch keine Bewertungen
- Etched Cast RestorationsDokument41 SeitenEtched Cast Restorationssharanya chekkarrajNoch keine Bewertungen
- Oral Hygiene Index-SimplifiedDokument36 SeitenOral Hygiene Index-SimplifiedKristina Robles50% (2)
- Demin/Remin in Preventive Dentistry: Demineralization By Foods, Acids, And Bacteria, And How To Counter Using RemineralizationVon EverandDemin/Remin in Preventive Dentistry: Demineralization By Foods, Acids, And Bacteria, And How To Counter Using RemineralizationNoch keine Bewertungen
- Facial NerveDokument128 SeitenFacial NervevaneetNoch keine Bewertungen
- Pulp Therapy of Non-Vital Teeth (Pulpectomy)Dokument27 SeitenPulp Therapy of Non-Vital Teeth (Pulpectomy)Mahmoud A. ZoghborNoch keine Bewertungen
- MDS Oral Medicine Question Papers 2002Dokument5 SeitenMDS Oral Medicine Question Papers 2002Niyas UmmerNoch keine Bewertungen
- Topic 1: © Aspire Training & ConsultingDokument20 SeitenTopic 1: © Aspire Training & ConsultingMashael SulimanNoch keine Bewertungen
- Operative DentistryDokument51 SeitenOperative Dentistryqra_beliebersNoch keine Bewertungen
- Clinical Evaluation of Abutment Teeth of Removable PartialDokument7 SeitenClinical Evaluation of Abutment Teeth of Removable PartialAlex KwokNoch keine Bewertungen
- Peridontal Pocket PerioDokument29 SeitenPeridontal Pocket PerioFourthMolar.comNoch keine Bewertungen
- CFPP 01-01C Final PDFDokument88 SeitenCFPP 01-01C Final PDFAndrey Cunha100% (1)
- Chapter 1Dokument38 SeitenChapter 1synap5esNoch keine Bewertungen
- Epidemiologi Dental CariesDokument21 SeitenEpidemiologi Dental CariesSampahAjaNoch keine Bewertungen
- Differences Between Natural Teeth & Dental ImplantsDokument19 SeitenDifferences Between Natural Teeth & Dental ImplantsLesta YangNoch keine Bewertungen
- DR Neeraj Gugnani - Ecc PDFDokument29 SeitenDR Neeraj Gugnani - Ecc PDFshailaja chintaNoch keine Bewertungen
- Vital Therapy in Carious ToothDokument9 SeitenVital Therapy in Carious ToothAsh PeiNoch keine Bewertungen
- Lecture 4 Diagnosis of Dental CariesDokument12 SeitenLecture 4 Diagnosis of Dental CariesDt omarNoch keine Bewertungen
- OMD411T - Oral Medicine 1Dokument117 SeitenOMD411T - Oral Medicine 1Noura Rihan100% (1)
- Periodontal Treatment in Medically CompromisedDokument14 SeitenPeriodontal Treatment in Medically CompromisedAbdallah Essam Al-ZireeniNoch keine Bewertungen
- Polyetheretherketone PEEK Dental Implants A Case FDokument8 SeitenPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- Mounting Dental X-RaysDokument6 SeitenMounting Dental X-RaysZahid AhmadNoch keine Bewertungen
- Restoration of Endodontically Treated TeethDokument33 SeitenRestoration of Endodontically Treated TeethHeng SiekhongNoch keine Bewertungen
- Conscious Sedation Guidelines for DentistsDokument18 SeitenConscious Sedation Guidelines for DentistsAnna NgNoch keine Bewertungen
- Non Cervical Lesions Meena MamDokument120 SeitenNon Cervical Lesions Meena Mamanshida v pNoch keine Bewertungen
- Apically Extruded Debris in Curved Root Canals Using A New Reciprocating Single-File Shaping SystemDokument6 SeitenApically Extruded Debris in Curved Root Canals Using A New Reciprocating Single-File Shaping SystemDANTE DELEGUERYNoch keine Bewertungen
- Causes of Endodontic FailuresDokument8 SeitenCauses of Endodontic Failuresizeldien5870Noch keine Bewertungen
- Failure of Endodontic Treatment: The Usual Suspects: ReviewDokument4 SeitenFailure of Endodontic Treatment: The Usual Suspects: ReviewTasyafikiNoch keine Bewertungen
- Classification of Dental CariesDokument80 SeitenClassification of Dental CariesOsman SoormaNoch keine Bewertungen
- Adhesion: Past, Present, and Future - Dental Asia - November/December 2019Dokument5 SeitenAdhesion: Past, Present, and Future - Dental Asia - November/December 2019pooja100% (1)
- GingivectomyDokument7 SeitenGingivectomyRirin SupriyaniNoch keine Bewertungen
- Class IV Composite Repair for Heavily Textured Central IncisorDokument8 SeitenClass IV Composite Repair for Heavily Textured Central IncisorventynataliaNoch keine Bewertungen
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDokument39 SeitenAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNoch keine Bewertungen
- Tooth Discolour at Ion PedoDokument28 SeitenTooth Discolour at Ion PedoFourthMolar.comNoch keine Bewertungen
- Dentistry: Primary Dental Care Services in England and WalesDokument72 SeitenDentistry: Primary Dental Care Services in England and WalesAyman BafaQeehNoch keine Bewertungen
- Traumatic Injuries Notes 22nk8pfDokument16 SeitenTraumatic Injuries Notes 22nk8pfAmee PatelNoch keine Bewertungen
- Coll, 2017Dokument13 SeitenColl, 2017Estaf EmkeyzNoch keine Bewertungen
- DR Nick Lekic - Space MaintainersDokument35 SeitenDR Nick Lekic - Space MaintainersanatomimanusiaNoch keine Bewertungen
- The Risk For Endocarditis in Dental PracticeDokument9 SeitenThe Risk For Endocarditis in Dental PracticeisanreryNoch keine Bewertungen
- Molar Incisor Hypomineralization Supplementary, Restorative, Orthodontic, and Esthetic Long-Term Treatment 2019Dokument6 SeitenMolar Incisor Hypomineralization Supplementary, Restorative, Orthodontic, and Esthetic Long-Term Treatment 2019player osamaNoch keine Bewertungen
- Mosby's Dental Drug ReferenceDokument3 SeitenMosby's Dental Drug ReferenceNada Gaafer Abdelrahim0% (1)
- A 100-Year Journey From GV Black To Minimal Surgical InterventionDokument6 SeitenA 100-Year Journey From GV Black To Minimal Surgical InterventionMichael XuNoch keine Bewertungen
- Development of OcclusionDokument49 SeitenDevelopment of OcclusionSardarni Ramandeep KaurNoch keine Bewertungen
- DentalDokument42 SeitenDentalmahesardarNoch keine Bewertungen
- Existing Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDokument47 SeitenExisting Restoration - Clinical Status: Secondary Caries Marginal Integrity Biomechanical FormDaniel WangNoch keine Bewertungen
- Vital Pulp Therapy in Vital Permanent Teeth With Cariously Exposed Pulp PDFDokument7 SeitenVital Pulp Therapy in Vital Permanent Teeth With Cariously Exposed Pulp PDFFabian ArangoNoch keine Bewertungen
- ClassificationDokument65 SeitenClassificationkharachi100% (1)
- Reducing The Risk of Failure Incomplete Denture PatientsDokument8 SeitenReducing The Risk of Failure Incomplete Denture PatientsHisyam IshakNoch keine Bewertungen
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDokument6 SeitenEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargNoch keine Bewertungen
- Denture Related StomatitisDokument8 SeitenDenture Related StomatitisLike OliviaNoch keine Bewertungen
- Dental AuxiliariesDokument14 SeitenDental AuxiliariesnainaNoch keine Bewertungen
- Tests For Biocompatibility of Dental MaterialsDokument151 SeitenTests For Biocompatibility of Dental MaterialsDevanshi SharmaNoch keine Bewertungen
- A Guide To Succeeding in The Df1 Interview (Sample Pages Only)Dokument15 SeitenA Guide To Succeeding in The Df1 Interview (Sample Pages Only)jaipald9067% (3)
- Rachel A Oakes 2019 ResumeDokument2 SeitenRachel A Oakes 2019 Resumeapi-455082100Noch keine Bewertungen
- Class II Composite Preparation & RestorationDokument12 SeitenClass II Composite Preparation & RestorationDavid ColonNoch keine Bewertungen
- Hyperbaric Oxygen Therapy For A Pediatric Electrical BurnDokument3 SeitenHyperbaric Oxygen Therapy For A Pediatric Electrical Burnsarah iriamanaNoch keine Bewertungen
- Sirshasana: Sirsasana 001 Sirsasana 002 Sirsasana 003 Sirsasana 004Dokument2 SeitenSirshasana: Sirsasana 001 Sirsasana 002 Sirsasana 003 Sirsasana 004Karisma SenapatiNoch keine Bewertungen
- Thesis List of EquationsDokument8 SeitenThesis List of Equationsfc5g0qm1100% (2)
- Mini Lecture Morphology of Skin LesionDokument48 SeitenMini Lecture Morphology of Skin LesionAlkaustariyah LubisNoch keine Bewertungen
- 07 Alkaline Phosphatase & Acid PhosphataseDokument12 Seiten07 Alkaline Phosphatase & Acid PhosphataseFrances FranciscoNoch keine Bewertungen
- The Human Body Frequency: March 2020Dokument3 SeitenThe Human Body Frequency: March 2020Dejya CordoraNoch keine Bewertungen
- Bioinformatics PaperDokument8 SeitenBioinformatics PaperrashigaurNoch keine Bewertungen
- Product Support Booklet: Lara Briden Endometriosis and PcosDokument24 SeitenProduct Support Booklet: Lara Briden Endometriosis and PcosVeronica TestaNoch keine Bewertungen
- When I hear the noiseDokument2 SeitenWhen I hear the noiseh00nguy0n-18Noch keine Bewertungen
- Asthma and COPDDokument79 SeitenAsthma and COPDDawit g/kidanNoch keine Bewertungen
- Discrimination Resource Dec. 2020Dokument33 SeitenDiscrimination Resource Dec. 2020Fiorella CastilloNoch keine Bewertungen
- Asphyxia Types and SignsDokument31 SeitenAsphyxia Types and SignsSita SilastutiNoch keine Bewertungen
- Case Study: Carol: By: Manpreet Kaur, Sarah Riley, Ben AvilaDokument14 SeitenCase Study: Carol: By: Manpreet Kaur, Sarah Riley, Ben AvilaBuchet AmalieNoch keine Bewertungen
- Maharlika Highway, Brgy. Magsaysay, Lopez, Quezon: Lopez National Comprehensive High SchoolDokument5 SeitenMaharlika Highway, Brgy. Magsaysay, Lopez, Quezon: Lopez National Comprehensive High SchoolJoenell CabungcalNoch keine Bewertungen
- Virulence: Factors in Escherichia Coli Urinary Tract InfectionDokument49 SeitenVirulence: Factors in Escherichia Coli Urinary Tract Infectionfajar nugrahaNoch keine Bewertungen
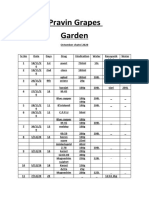
- Pravin Grapes Garden Octomber chatni 2020 recordsDokument9 SeitenPravin Grapes Garden Octomber chatni 2020 recordsPravin ShindeNoch keine Bewertungen
- Unstd-Com 4268 Vegetable Radish FreshDokument2 SeitenUnstd-Com 4268 Vegetable Radish FreshOzlem MepNoch keine Bewertungen
- Arachnoid Granulations PDFDokument5 SeitenArachnoid Granulations PDFsebacosNoch keine Bewertungen
- Pill CameraDokument21 SeitenPill CameraAnil DsouzaNoch keine Bewertungen
- Ocumentation: Analysis of The Situation and Trends in Sunscreen ProductsDokument4 SeitenOcumentation: Analysis of The Situation and Trends in Sunscreen ProductsEvelyn GómezNoch keine Bewertungen
- Quick Guide For BS200Dokument16 SeitenQuick Guide For BS200Diego Manuel TernidaNoch keine Bewertungen