Das könnte Ihnen auch gefallen
- Eneroth H, Persson L-Å, El Arifeen S, Ekström E-C. InfantDokument6 SeitenEneroth H, Persson L-Å, El Arifeen S, Ekström E-C. Infantaflah alfaNoch keine Bewertungen
- 1 s2.0 S0899900714005498 MainDokument6 Seiten1 s2.0 S0899900714005498 MainKomala SariNoch keine Bewertungen
- JURDING Feritin SerumDokument11 SeitenJURDING Feritin SerumTasya LaresaNoch keine Bewertungen
- Daily Consumption of Growing-Up Milk Is Associated With Less Stunting Among Indonesian ToddlersDokument7 SeitenDaily Consumption of Growing-Up Milk Is Associated With Less Stunting Among Indonesian ToddlersAnugerah DestiaNoch keine Bewertungen
- Building A Prediction Model FoDokument9 SeitenBuilding A Prediction Model Fosyukrianti syahdaNoch keine Bewertungen
- Arch Dis Child 2005 Aggarwal 26 9Dokument5 SeitenArch Dis Child 2005 Aggarwal 26 9Dyera JessenskyNoch keine Bewertungen
- Clinica Chimica ActaDokument6 SeitenClinica Chimica ActaNovita DewiNoch keine Bewertungen
- Low Iron Stores in Preconception Nulliparous Women A Two Center - 2020 - NutriDokument5 SeitenLow Iron Stores in Preconception Nulliparous Women A Two Center - 2020 - NutriRinaNoch keine Bewertungen
- Artikel 2Dokument7 SeitenArtikel 2Claudia BuheliNoch keine Bewertungen
- Wu 2013Dokument16 SeitenWu 2013Maykelly da Silva GomesNoch keine Bewertungen
- Maternal Vitamin B 12 StatusDokument10 SeitenMaternal Vitamin B 12 StatusReyes Ivan García CuevasNoch keine Bewertungen
- Jeumpa Syahrana Salsabila-BalitaDokument10 SeitenJeumpa Syahrana Salsabila-BalitaMetha IerayanaNoch keine Bewertungen
- Nutrition For Late Preterm Babies What Should We Know.Dokument25 SeitenNutrition For Late Preterm Babies What Should We Know.IKA UNAIRNoch keine Bewertungen
- AnemiaDokument8 SeitenAnemiaLaluNoch keine Bewertungen
- Oxid ST 1Dokument7 SeitenOxid ST 1Mohamed HussienNoch keine Bewertungen
- Cormack 2021 - Neonatal Refeeding Syndrome and Clinical Outcome in ELBW Secondary Cohort Analysis ProVIDe TrialDokument14 SeitenCormack 2021 - Neonatal Refeeding Syndrome and Clinical Outcome in ELBW Secondary Cohort Analysis ProVIDe TrialKarla LapendaNoch keine Bewertungen
- The Effect of Bovine Colostrum/egg Supplementation Compared With Corn/soy Flour in Young Malawian Children: A Randomized, Controlled Clinical TrialDokument8 SeitenThe Effect of Bovine Colostrum/egg Supplementation Compared With Corn/soy Flour in Young Malawian Children: A Randomized, Controlled Clinical TrialSukma DewiNoch keine Bewertungen
- Directiva Suplementacion 2016 AnemiaDokument11 SeitenDirectiva Suplementacion 2016 AnemiaJose Luis Marin CatacoraNoch keine Bewertungen
- 840Dokument8 Seiten840Ari YulistiNoch keine Bewertungen
- Role of Sodium and Potassium Ions in Identification of Offspring Gender in RatsDokument6 SeitenRole of Sodium and Potassium Ions in Identification of Offspring Gender in RatsIOSR Journal of PharmacyNoch keine Bewertungen
- Iron and Folic Acid Supplements and Reduced Early Neonatal Deaths in IndonesiaDokument10 SeitenIron and Folic Acid Supplements and Reduced Early Neonatal Deaths in IndonesiaIlvita MayasariNoch keine Bewertungen
- 17 Gibson 2017Dokument9 Seiten17 Gibson 2017Dinda Asa AyukhalizaNoch keine Bewertungen
- Adverse Effects of Iron Deficiency Anemia On Pregnancy Outcome and Offspring Development and Intervention of Three Iron SupplementsDokument11 SeitenAdverse Effects of Iron Deficiency Anemia On Pregnancy Outcome and Offspring Development and Intervention of Three Iron SupplementsAjay DNoch keine Bewertungen
- Comparison of Oral Versus Injectable Vitamin-D For The Treatment of Nutritional Vitamin-D Deficiency RicketsDokument4 SeitenComparison of Oral Versus Injectable Vitamin-D For The Treatment of Nutritional Vitamin-D Deficiency RicketsMultan SohanhalwaNoch keine Bewertungen
- Iron and Folic Acid Supplements and Reduced Early Neonatal Deaths in IndonesiaDokument10 SeitenIron and Folic Acid Supplements and Reduced Early Neonatal Deaths in Indonesiarobby zayendraNoch keine Bewertungen
- Kriteria Rawat IcuDokument6 SeitenKriteria Rawat Icuriska sovinaNoch keine Bewertungen
- Effective Interventions To Address Maternal and Child Malnutrition: An Update of The EvidenceDokument18 SeitenEffective Interventions To Address Maternal and Child Malnutrition: An Update of The EvidenceChris ValNoch keine Bewertungen
- Paediatrica Indonesiana: Kadek Wini Mardewi, I Gusti Lanang Sidiartha, Eka GunawijayaDokument5 SeitenPaediatrica Indonesiana: Kadek Wini Mardewi, I Gusti Lanang Sidiartha, Eka GunawijayaLala AkamatsuNoch keine Bewertungen
- Rahayu & Wahyu, 2021Dokument8 SeitenRahayu & Wahyu, 2021Chingura LuffyNoch keine Bewertungen
- Pregnancy 1Dokument12 SeitenPregnancy 1Toni FauziNoch keine Bewertungen
- Is There An Association Between Vitamin D Level and IronDokument7 SeitenIs There An Association Between Vitamin D Level and IronRandy SuryawanNoch keine Bewertungen
- WJG 14 6133 PDFDokument7 SeitenWJG 14 6133 PDFSugiantoNoch keine Bewertungen
- Effect of Vitamin D Supplementation and Calcium in Reducing The Risk of Preeclampsia: Meta-AnalysisDokument13 SeitenEffect of Vitamin D Supplementation and Calcium in Reducing The Risk of Preeclampsia: Meta-AnalysisAldo TanNoch keine Bewertungen
- Vitamin DDokument11 SeitenVitamin DCastiglianoNoch keine Bewertungen
- Bhutta Interventions LCAH 2021Dokument18 SeitenBhutta Interventions LCAH 2021Angelica EstipularNoch keine Bewertungen
- Pone 0117038 PDFDokument20 SeitenPone 0117038 PDFAmalia Dwi AryantiNoch keine Bewertungen
- ZEMEL, Kebutuhan Kalsium AnakDokument2 SeitenZEMEL, Kebutuhan Kalsium AnakAzizah Sabrina 19 057Noch keine Bewertungen
- Jurnal Internasional Q3Dokument5 SeitenJurnal Internasional Q3AlfaniNoch keine Bewertungen
- Nutritional Managment of Newborn Infants Practical Guidelines 2008Dokument7 SeitenNutritional Managment of Newborn Infants Practical Guidelines 2008aweisgarberNoch keine Bewertungen
- Adgent Et Al - 2018 - A Longitudinal Study of Estrogen-Responsive Tissues and Hormone ConcentrationsDokument11 SeitenAdgent Et Al - 2018 - A Longitudinal Study of Estrogen-Responsive Tissues and Hormone ConcentrationsBerry BancinNoch keine Bewertungen
- Journal Pmed 1003122Dokument25 SeitenJournal Pmed 1003122ayi chrisenggarNoch keine Bewertungen
- 2008 - QUIGLEY Et Al - Effect of Variable Long-Term Maternal Feed Allowance On The Development of The Ovine Placenta and FetusDokument10 Seiten2008 - QUIGLEY Et Al - Effect of Variable Long-Term Maternal Feed Allowance On The Development of The Ovine Placenta and FetusSamanta MonteiroNoch keine Bewertungen
- 103 The Relationship Between Nursing Pattern &, Breast Milk Intake in The First Year of LifeDokument1 Seite103 The Relationship Between Nursing Pattern &, Breast Milk Intake in The First Year of LifeDaniella AwurumibeNoch keine Bewertungen
- Lesson Plan 4 Powerpoint 4 2Dokument21 SeitenLesson Plan 4 Powerpoint 4 2api-523266509100% (1)
- RandomizedDokument7 SeitenRandomizedmechi_ghisyaNoch keine Bewertungen
- JAMA Ophthalmology Volume Issue 2018 (Doi 10.1001 - Jamaophthalmol.2018.2753) Binenbaum, Gil Bell, Edward F. Donohue, Pamela Quinn, Graham - Development of Modified Screening Criteria For Retinop PDFDokument7 SeitenJAMA Ophthalmology Volume Issue 2018 (Doi 10.1001 - Jamaophthalmol.2018.2753) Binenbaum, Gil Bell, Edward F. Donohue, Pamela Quinn, Graham - Development of Modified Screening Criteria For Retinop PDFKarthik CNoch keine Bewertungen
- Iron Supplementation of Breastfed Infants From An Early Age: See Corresponding Editorial On Page 473Dokument8 SeitenIron Supplementation of Breastfed Infants From An Early Age: See Corresponding Editorial On Page 473Kania A BustamNoch keine Bewertungen
- Iron Deficiency in Young Children: A Risk Marker For Early Childhood CariesDokument6 SeitenIron Deficiency in Young Children: A Risk Marker For Early Childhood Carieswahyudi_donnyNoch keine Bewertungen
- Knowledge, Attitude and Practice Related To Iron Deficiency Anemia Among Women of Child Bearing Age, Khartoum, SudanDokument7 SeitenKnowledge, Attitude and Practice Related To Iron Deficiency Anemia Among Women of Child Bearing Age, Khartoum, SudanInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Martial of Hypotrophe To Lubumbashi Factors Maternal Associated With Neonatal HypoferritinemiaDokument14 SeitenMartial of Hypotrophe To Lubumbashi Factors Maternal Associated With Neonatal HypoferritinemiaInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Jurnal Endokrin 1Dokument14 SeitenJurnal Endokrin 1Devi Boru Panggoaran SitinjakNoch keine Bewertungen
- Am J Clin Nutr-2013-Abrams-1373-4 Zinc For Preterm Infants, Who Needs It and How Much Is Needed PDFDokument2 SeitenAm J Clin Nutr-2013-Abrams-1373-4 Zinc For Preterm Infants, Who Needs It and How Much Is Needed PDFKhalila DiantiNoch keine Bewertungen
- Risk Factors For Nutritional Rickets in Children of Northern KeralaDokument3 SeitenRisk Factors For Nutritional Rickets in Children of Northern KeralaInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Jurnal BayiDokument7 SeitenJurnal BayiAnonymous AKr7hWjBiNoch keine Bewertungen
- Lancet Iodo GestantesDokument7 SeitenLancet Iodo GestantesMarcos VinicioNoch keine Bewertungen
- Clinical Nutrition: Aisha Mansoor Ali, Abdulaziz Alobaid, Tasnim Nidal Malhis, Ahmad Fawzi KhattabDokument7 SeitenClinical Nutrition: Aisha Mansoor Ali, Abdulaziz Alobaid, Tasnim Nidal Malhis, Ahmad Fawzi KhattabDewi Retno AstutyNoch keine Bewertungen
- Literature Review On Protein Energy MalnutritionDokument8 SeitenLiterature Review On Protein Energy Malnutritionafdttjujo100% (1)
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsVon EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNoch keine Bewertungen
- Global Landscape of Nutrition Challenges in Infants and ChildrenVon EverandGlobal Landscape of Nutrition Challenges in Infants and ChildrenNoch keine Bewertungen
- LO Week 5 Tutorial 2Dokument7 SeitenLO Week 5 Tutorial 2Hizkia MarlissaNoch keine Bewertungen
- Biokimia Sistem Hematologi EnglishDokument46 SeitenBiokimia Sistem Hematologi EnglishIrham KhairiNoch keine Bewertungen
- Marcia's Brain Based Learning HandoutsDokument27 SeitenMarcia's Brain Based Learning HandoutsBadaruddin SappaNoch keine Bewertungen
- Olfactory Colours and Coloured SmellsDokument28 SeitenOlfactory Colours and Coloured Smellsspa100% (2)
- CBSE Class 10 Science Chapter 6 Important Questions With SolutionsDokument48 SeitenCBSE Class 10 Science Chapter 6 Important Questions With SolutionsRohit ChouhanNoch keine Bewertungen
- NZ Wood Design GuidesDokument48 SeitenNZ Wood Design GuidesHiệp Nguyễn VănNoch keine Bewertungen
- Lab ReportDokument6 SeitenLab ReportJenniferNoch keine Bewertungen
- Science SNC2D Grade 10 ExamDokument8 SeitenScience SNC2D Grade 10 ExamRiazNoch keine Bewertungen
- Case Study 1-BwilliamsDokument3 SeitenCase Study 1-Bwilliamsapi-336564677Noch keine Bewertungen
- Crittenden Ainsworth 1989 PDFDokument32 SeitenCrittenden Ainsworth 1989 PDFHalima MarthaNoch keine Bewertungen
- 17 3Dokument30 Seiten17 3Lim ZjianNoch keine Bewertungen
- Use of Dinitrosalicylic Acid Reagent For Determination of Reducing SugarDokument7 SeitenUse of Dinitrosalicylic Acid Reagent For Determination of Reducing SugarLANANoch keine Bewertungen
- Why Are Elephants Less Likely To Get CancerDokument8 SeitenWhy Are Elephants Less Likely To Get Canceralicia tNoch keine Bewertungen
- Bodytalk Fundamentals: Getting Familiar With The Charts. Photo Credit: Charlotte NielsenDokument22 SeitenBodytalk Fundamentals: Getting Familiar With The Charts. Photo Credit: Charlotte Nielsenmelina jamesNoch keine Bewertungen
- Low-Cycle Fatigue Behavior of 3d-Printed PLA-based Porous ScaffoldsDokument8 SeitenLow-Cycle Fatigue Behavior of 3d-Printed PLA-based Porous ScaffoldskaminaljuyuNoch keine Bewertungen
- Biology P&DDokument5 SeitenBiology P&DMakeedaNoch keine Bewertungen
- Capsule Research ProposalDokument13 SeitenCapsule Research ProposalTomas John T. GuzmanNoch keine Bewertungen
- Mairet Philippe - Alfred Adler Problems of Neuro PDFDokument217 SeitenMairet Philippe - Alfred Adler Problems of Neuro PDFRadu Prusan100% (1)
- JGXP - 2011 - v15n4 - Contamination Control in The Compliance Program PDFDokument7 SeitenJGXP - 2011 - v15n4 - Contamination Control in The Compliance Program PDFNelson Alejandro FierroNoch keine Bewertungen
- Shimelis WondimuDokument95 SeitenShimelis WondimuMelaku MamayeNoch keine Bewertungen
- Inheritance 14.2Dokument6 SeitenInheritance 14.2YashodhaNoch keine Bewertungen
- On The Purpose of A Liberal Arts EducationDokument9 SeitenOn The Purpose of A Liberal Arts EducationSyairah Banu DjufriNoch keine Bewertungen
- Peppered Moth Gizmo - Answer KeyDokument4 SeitenPeppered Moth Gizmo - Answer KeyDareea Tate30% (10)
- Campbell Biology - Chapters 1 Ans 2 SummaryDokument17 SeitenCampbell Biology - Chapters 1 Ans 2 SummaryYana JohansonNoch keine Bewertungen
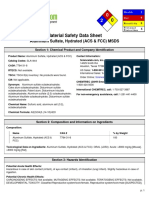
- Aluminum Sulfate, Hydrated (ACS & FCC) MSDS: Section 1: Chemical Product and Company IdentificationDokument6 SeitenAluminum Sulfate, Hydrated (ACS & FCC) MSDS: Section 1: Chemical Product and Company IdentificationBintang Benarivo MangengkeNoch keine Bewertungen
- TIMEMANAGEMENTDokument13 SeitenTIMEMANAGEMENTPolinda UseroNoch keine Bewertungen
- SOF Level 2 NSO Class 3 PDFDokument5 SeitenSOF Level 2 NSO Class 3 PDFparesh_dhakeNoch keine Bewertungen
- 23andme and The FDADokument4 Seiten23andme and The FDAChristodoulos DolapsakisNoch keine Bewertungen
- A 6 Years Old Girl With Intraabdomen TB, Severe Chronic Malnutrition, Post Exploration Laparotomy+Right Hemiileoctomy+ Ileocaecal AnastomosisDokument26 SeitenA 6 Years Old Girl With Intraabdomen TB, Severe Chronic Malnutrition, Post Exploration Laparotomy+Right Hemiileoctomy+ Ileocaecal AnastomosisNadia ChairunnisaNoch keine Bewertungen
- BirknerDokument40 SeitenBirknerSylvain ContiéNoch keine Bewertungen