Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Starfish PrimeDokument31 SeitenStarfish PrimeonatbrossNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Disaster Recovery PlanDokument22 SeitenDisaster Recovery PlanOsama100% (2)
- Aircraft General Multiple-Choice Exercise for B737 Cockpit ProceduresDokument11 SeitenAircraft General Multiple-Choice Exercise for B737 Cockpit ProceduresKhurram NaseemNoch keine Bewertungen
- Boiler EmergenciesDokument15 SeitenBoiler EmergenciesAmit ChauhanNoch keine Bewertungen
- Disaster Is "A Sudden, Calamitous Occurrence That Causes Great Harm, InjuryDokument12 SeitenDisaster Is "A Sudden, Calamitous Occurrence That Causes Great Harm, InjuryRalph Louis RosarioNoch keine Bewertungen
- Basic Concept in Disaster ManagementDokument18 SeitenBasic Concept in Disaster ManagementSagar ParateNoch keine Bewertungen
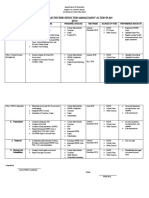
- School Disaster Risk Reduction Management Action Plan 2019Dokument2 SeitenSchool Disaster Risk Reduction Management Action Plan 2019Maricris Baldespinosa100% (3)
- Chapter 12. FEMA 751-TextoDokument64 SeitenChapter 12. FEMA 751-TextoPaul RuizNoch keine Bewertungen
- Emergency Warden Training For ADDokument20 SeitenEmergency Warden Training For ADsetiawanaji407Noch keine Bewertungen
- DRILL MATRIX Annex 9.2 PDFDokument4 SeitenDRILL MATRIX Annex 9.2 PDFNaNNoch keine Bewertungen
- 01 GDL Suhartatik 1184 1 Artikel SDokument6 Seiten01 GDL Suhartatik 1184 1 Artikel SayuNoch keine Bewertungen
- 1683 4152 1 PBDokument8 Seiten1683 4152 1 PBayuNoch keine Bewertungen
- Makalah Bahasa InggrisDokument10 SeitenMakalah Bahasa InggrisayuNoch keine Bewertungen
- 106 31 1 PB PDFDokument6 Seiten106 31 1 PB PDFAi NdriNoch keine Bewertungen
- 24-Article Text-115-1-10-20141210Dokument7 Seiten24-Article Text-115-1-10-20141210ayuNoch keine Bewertungen
- English 105 "Dietary Program To Diabetus Melitus": Academic: I'IN NOVIANA M.PDDokument14 SeitenEnglish 105 "Dietary Program To Diabetus Melitus": Academic: I'IN NOVIANA M.PDayuNoch keine Bewertungen
- Poslen: (Talinun Triangular (Jacq J Willd) )Dokument2 SeitenPoslen: (Talinun Triangular (Jacq J Willd) )ayuNoch keine Bewertungen
- Trilogi Dalam Membangun Sekolah UnggulDokument12 SeitenTrilogi Dalam Membangun Sekolah UnggulayuNoch keine Bewertungen
- 20 35 2 PB PDFDokument9 Seiten20 35 2 PB PDFYenika AgustinaNoch keine Bewertungen
- Makalah BingDokument13 SeitenMakalah BingayuNoch keine Bewertungen
- B InggrisDokument6 SeitenB InggrisayuNoch keine Bewertungen
- John Legend All of Me LyricsDokument3 SeitenJohn Legend All of Me LyricsayuNoch keine Bewertungen
- Bahan B AnisDokument1 SeiteBahan B AnisayuNoch keine Bewertungen
- B InggrisDokument6 SeitenB InggrisayuNoch keine Bewertungen
- Disaster Risk Reduction and ManagementDokument18 SeitenDisaster Risk Reduction and ManagementMichelle AposagaNoch keine Bewertungen
- Mapping Risks at Ramon M. Durano Sr. FoundationDokument14 SeitenMapping Risks at Ramon M. Durano Sr. FoundationYan EscotonNoch keine Bewertungen
- Casualty EvacuationDokument29 SeitenCasualty Evacuationdibera18Noch keine Bewertungen
- A320 FCOM Vol 1 ISS Rev 43DDokument1.337 SeitenA320 FCOM Vol 1 ISS Rev 43DRiccardo Casarosa0% (1)
- Falls Risk Interventions GuideDokument1 SeiteFalls Risk Interventions GuidePuja PatelNoch keine Bewertungen
- Longford ExplosionDokument2 SeitenLongford ExplosionZalu PrasetyoNoch keine Bewertungen
- DRRMDokument27 SeitenDRRMYochabel Eureca BorjeNoch keine Bewertungen
- Training - Tsunami Hazard and Vulnerability For Decision Makers Planners and Managers of Coastal Infrastructure PDFDokument116 SeitenTraining - Tsunami Hazard and Vulnerability For Decision Makers Planners and Managers of Coastal Infrastructure PDFCDMP BangladeshNoch keine Bewertungen
- PM 002j FAST1 Trainers ManualDokument32 SeitenPM 002j FAST1 Trainers ManualjohnnicholasrosettiNoch keine Bewertungen
- Cyclone AltheaDokument8 SeitenCyclone AltheaKostas VlahosNoch keine Bewertungen
- Multidisciplinary and Quarterly Self Inspection: Environmental Rounds ChecklistDokument12 SeitenMultidisciplinary and Quarterly Self Inspection: Environmental Rounds Checklistshilpa ksNoch keine Bewertungen
- Business Continuity Planning at The Bank of JapanDokument11 SeitenBusiness Continuity Planning at The Bank of Japanblue_l1Noch keine Bewertungen
- DPPM Unit 1 Study MaterialDokument46 SeitenDPPM Unit 1 Study MaterialJyothi GNoch keine Bewertungen
- Attendance Sheet For EvacuationDokument10 SeitenAttendance Sheet For EvacuationSALGIE SERNALNoch keine Bewertungen
- Post-Activity Report Eoc TrainingDokument25 SeitenPost-Activity Report Eoc TrainingKATHLEEN PONCE COCHARONoch keine Bewertungen
- Natural Disaster Scavenger HuntDokument4 SeitenNatural Disaster Scavenger Huntapi-279520270Noch keine Bewertungen
- Risk Assessment Film TrailerDokument1 SeiteRisk Assessment Film TrailerZara MartincevicNoch keine Bewertungen
- Thesis Ahmad Reza DjalaliDokument92 SeitenThesis Ahmad Reza DjalaliNaviin KrishnanNoch keine Bewertungen
- 02-2014 Graciano Banaga LotDokument2 Seiten02-2014 Graciano Banaga LotSbGuinobatanNoch keine Bewertungen
- Quick Inspection Manual of Damaged Reinforced Concrete Buildings Due To Earthquakes (Govt. of Japan)Dokument52 SeitenQuick Inspection Manual of Damaged Reinforced Concrete Buildings Due To Earthquakes (Govt. of Japan)TuanQuachNoch keine Bewertungen