Das könnte Ihnen auch gefallen
- Clinical Clues With Urogenital SyndromeDokument3 SeitenClinical Clues With Urogenital Syndromemefav7778520Noch keine Bewertungen
- US Hypertension Review GuidelinesDokument12 SeitenUS Hypertension Review Guidelinesmefav7778520100% (1)
- Urethritis Testing and TX GuidelinesDokument2 SeitenUrethritis Testing and TX Guidelinesmefav7778520Noch keine Bewertungen
- Bell's Palsy - Differential Diagnosis of Facial Nerve PalsyDokument2 SeitenBell's Palsy - Differential Diagnosis of Facial Nerve Palsymefav7778520Noch keine Bewertungen
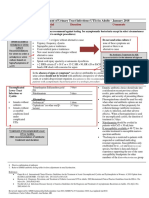
- Acute Gout ManagementDokument2 SeitenAcute Gout Managementmefav7778520Noch keine Bewertungen
- Algorithm of Acute GoutDokument2 SeitenAlgorithm of Acute Goutmefav7778520Noch keine Bewertungen
- Bell's Palsy - Facial Nerve and Supranuclear LesionDokument1 SeiteBell's Palsy - Facial Nerve and Supranuclear Lesionmefav7778520Noch keine Bewertungen
- Purine Foods ContentDokument1 SeitePurine Foods Contentmefav7778520Noch keine Bewertungen
- Bell's Palsy - Anatomy of Facial NerveDokument1 SeiteBell's Palsy - Anatomy of Facial Nervemefav7778520Noch keine Bewertungen
- Autism's Top 14 Areas of ConcernDokument2 SeitenAutism's Top 14 Areas of Concernmefav7778520Noch keine Bewertungen
- UTI Guideline Example 2 Appendix B PDFDokument4 SeitenUTI Guideline Example 2 Appendix B PDFamira catriNoch keine Bewertungen
- ER MEDS LIST WITH COMMON DRUGSDokument3 SeitenER MEDS LIST WITH COMMON DRUGSmefav7778520Noch keine Bewertungen
- Angular Cheilitis - Causes, Symptoms, Treatment and MoreDokument7 SeitenAngular Cheilitis - Causes, Symptoms, Treatment and Moremefav7778520Noch keine Bewertungen
- Wms GINA 2017 Main Report Tracked Changes For Archive PDFDokument156 SeitenWms GINA 2017 Main Report Tracked Changes For Archive PDFAnnisa MiendaNoch keine Bewertungen
- Bell's Palsy: Diagnosis and ManagementDokument2 SeitenBell's Palsy: Diagnosis and Managementmefav7778520Noch keine Bewertungen
- Instituting CHANGE in The WorkplaceDokument39 SeitenInstituting CHANGE in The Workplacemefav7778520Noch keine Bewertungen
- Emergency Preparedness (Zap)Dokument24 SeitenEmergency Preparedness (Zap)adel santosNoch keine Bewertungen
- TB in The WorkplaceDokument60 SeitenTB in The Workplacemefav7778520100% (1)
- Industrial HygieneDokument111 SeitenIndustrial Hygienemefav7778520100% (1)
- Do 53-03Dokument6 SeitenDo 53-03mefav7778520Noch keine Bewertungen
- Drug Free WorkplaceDokument91 SeitenDrug Free Workplacemefav7778520Noch keine Bewertungen
- Electrical SafetyDokument35 SeitenElectrical Safetymefav7778520Noch keine Bewertungen
- Compensation MedicineDokument46 SeitenCompensation Medicinemefav7778520Noch keine Bewertungen
- Comprehensive and Unified Policy PDFDokument180 SeitenComprehensive and Unified Policy PDFmefav7778520Noch keine Bewertungen
- Accident CausationDokument104 SeitenAccident Causationmefav7778520Noch keine Bewertungen
- 5S Industrial HousekeepingDokument17 Seiten5S Industrial Housekeepingmefav7778520Noch keine Bewertungen
- Basic Concept On Toxicology PDFDokument40 SeitenBasic Concept On Toxicology PDFmefav7778520Noch keine Bewertungen
- Accident InvestigationDokument39 SeitenAccident Investigationmefav7778520Noch keine Bewertungen
- Ococ Notes PDFDokument5 SeitenOcoc Notes PDFmefav7778520Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Ir Jajad KaokabDokument13 SeitenIr Jajad Kaokabdharsa plyNoch keine Bewertungen
- ECG Masters' Collection Volume 2Dokument218 SeitenECG Masters' Collection Volume 2Илија Радосављевић100% (1)
- Pathophysiology of Hypertension: RAAS Activation and Organ DamageDokument2 SeitenPathophysiology of Hypertension: RAAS Activation and Organ DamageAlvin RamirezNoch keine Bewertungen
- Lecture On Atrial Pressure Changes and JVP by Dr. RoomiDokument9 SeitenLecture On Atrial Pressure Changes and JVP by Dr. RoomiMudassar Roomi100% (2)
- Nuclear Cases SummaryDokument106 SeitenNuclear Cases SummaryAkramNoch keine Bewertungen
- Congestive Heart FailureDokument25 SeitenCongestive Heart FailuredevianiamalinaNoch keine Bewertungen
- A Soft Total Artificial Heart-First Concept Evaluation OnDokument11 SeitenA Soft Total Artificial Heart-First Concept Evaluation OnSeyit Hamza ÇavgaNoch keine Bewertungen
- ICU Guideline: Temporary Cardiac PacingDokument8 SeitenICU Guideline: Temporary Cardiac PacingistiNoch keine Bewertungen
- ACLS Pre Test AnswersDokument10 SeitenACLS Pre Test AnswersAirene SibleNoch keine Bewertungen
- Emergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Dokument51 SeitenEmergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Lely Yuniarti AhqafNoch keine Bewertungen
- Implanted Cardioverter Defibrillator (Icd) Identification - : Wallet CardDokument1 SeiteImplanted Cardioverter Defibrillator (Icd) Identification - : Wallet CardΑλεξης ΝεοφυτουNoch keine Bewertungen
- Physiology of Heart in DetailDokument101 SeitenPhysiology of Heart in Detailakanksha sharmaNoch keine Bewertungen
- Zoll M Series Defibrillator Manual PDFDokument111 SeitenZoll M Series Defibrillator Manual PDFAhmad TanveerNoch keine Bewertungen
- Blood Pressure - Lab-FalconDokument9 SeitenBlood Pressure - Lab-FalconSebastián PérezNoch keine Bewertungen
- NCP (Coronary Artery Disease) - PacateDokument7 SeitenNCP (Coronary Artery Disease) - PacateKristile Ann PacateNoch keine Bewertungen
- Right Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Dokument9 SeitenRight Atrial Pressure in The Critically Ill: How To Measure, What Is The Value, What Are The Limitations?Trần Quang HuyNoch keine Bewertungen
- Preload and AfterloadDokument4 SeitenPreload and AfterloadNeranga SamaratungeNoch keine Bewertungen
- Introduction To ECG Interpretation January 2023Dokument101 SeitenIntroduction To ECG Interpretation January 2023davidjoejoekidNoch keine Bewertungen
- 3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CDokument65 Seiten3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CAlexa GoteraNoch keine Bewertungen
- Body Fluids and CirculationDokument10 SeitenBody Fluids and CirculationFree4TechNoch keine Bewertungen
- Intern TutorialDokument288 SeitenIntern TutorialtoffeepolNoch keine Bewertungen
- Cardiac Ultrasound Imaging ProtocolDokument152 SeitenCardiac Ultrasound Imaging Protocolbashir019Noch keine Bewertungen
- Basic ECG Interpretation 20-Question Practice TestDokument7 SeitenBasic ECG Interpretation 20-Question Practice Testemmaaziz100% (1)
- Atrial Fibrillation and Congestive Heart Failure: EditorialDokument3 SeitenAtrial Fibrillation and Congestive Heart Failure: EditorialfederikarosilawatiNoch keine Bewertungen
- Lab ManualDokument19 SeitenLab ManualShafin FinaNoch keine Bewertungen
- LESSON PLAN HypertensionDokument9 SeitenLESSON PLAN HypertensionARUN JOSE (08156864174)85% (39)
- ACLS Study Guide NewDokument35 SeitenACLS Study Guide NewNIRANJANA SHALININoch keine Bewertungen
- Perbandingan Tekanan Darah Sistolik Dan Diastolik Sebelum Dan Sesudah Begadang Pada DI Perumahan J-City Medan JohorDokument7 SeitenPerbandingan Tekanan Darah Sistolik Dan Diastolik Sebelum Dan Sesudah Begadang Pada DI Perumahan J-City Medan JohorDimas Angga PutraNoch keine Bewertungen
- Atrial Flutter & Fibrillation ExplainedDokument8 SeitenAtrial Flutter & Fibrillation ExplainedthomasfelixNoch keine Bewertungen
- Almostadoctor - co.Uk-Summary of ECG AbnormalitiesDokument8 SeitenAlmostadoctor - co.Uk-Summary of ECG AbnormalitiesAnu SharmaNoch keine Bewertungen