Das könnte Ihnen auch gefallen
- ( ) Temperature Agreed Between Supermetanol and SnamprogettiDokument1 Seite( ) Temperature Agreed Between Supermetanol and SnamprogettiluisNoch keine Bewertungen
- Electronegativity ChartDokument2 SeitenElectronegativity ChartDana FransenNoch keine Bewertungen
- Portfolio SnapshotDokument63 SeitenPortfolio Snapshotgurudev21Noch keine Bewertungen
- Method For Isolating Rna From Adipose TissueDokument7 SeitenMethod For Isolating Rna From Adipose TissueMark BaronNoch keine Bewertungen
- Frequencies: StatisticsDokument23 SeitenFrequencies: StatisticsKAiiiiNoch keine Bewertungen
- Report On Separation of Nitrogenous Substances.: Associate Referee?Dokument7 SeitenReport On Separation of Nitrogenous Substances.: Associate Referee?davidcasNoch keine Bewertungen
- Full Download Solution Manual For Dosage Calculations A Multi Method Approach 0132158620 PDF Full ChapterDokument35 SeitenFull Download Solution Manual For Dosage Calculations A Multi Method Approach 0132158620 PDF Full Chapterbradleywardxg7pz0100% (18)
- Stratma Matrices SHELLDokument34 SeitenStratma Matrices SHELLAngel Pido50% (2)
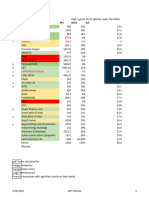
- Foodlog Date Febraury 42024 - Daily Intake 1Dokument1 SeiteFoodlog Date Febraury 42024 - Daily Intake 1api-732595195Noch keine Bewertungen
- Febuary 1 - Sheet1Dokument1 SeiteFebuary 1 - Sheet1api-447547104Noch keine Bewertungen
- Relations Between Erratic Engine Revolution and Diesel Fuel Lubricating PropertiesDokument3 SeitenRelations Between Erratic Engine Revolution and Diesel Fuel Lubricating PropertiesRahmid Farezi 1707111363Noch keine Bewertungen
- SafjbskdbfkDokument3 SeitenSafjbskdbfkYashpal MishraNoch keine Bewertungen
- Berliana Sari (FR)Dokument14 SeitenBerliana Sari (FR)berlianaNoch keine Bewertungen
- Food Log Date 220125Dokument4 SeitenFood Log Date 220125api-593711305Noch keine Bewertungen
- Organic Volatile Impurities - Retention Time IndexDokument6 SeitenOrganic Volatile Impurities - Retention Time IndexAmineJaouedNoch keine Bewertungen
- Cortante Basal Y Espectro De Diseño Nec 2015 Ubicación S. Estructural Suelo Opcupación Z (%g) Fa Fd Fs η r TDokument13 SeitenCortante Basal Y Espectro De Diseño Nec 2015 Ubicación S. Estructural Suelo Opcupación Z (%g) Fa Fd Fs η r TLizz VillacresNoch keine Bewertungen
- Saturator Circulation Water Hydrogenated Natural Gas Hydrogenated Natural Gas Natural Gas To Compressor IDDokument1 SeiteSaturator Circulation Water Hydrogenated Natural Gas Hydrogenated Natural Gas Natural Gas To Compressor IDluisNoch keine Bewertungen
- Chapters List WEIGHTAGEDokument3 SeitenChapters List WEIGHTAGEVISHNU PRIYA BUDDANINoch keine Bewertungen
- Source: Hydrology and Water Resources System For IndiaDokument2 SeitenSource: Hydrology and Water Resources System For IndiaPedroNoch keine Bewertungen
- Mirae Asset Global Electric & Autonomous Vehicles ETFs Fund of FundDokument20 SeitenMirae Asset Global Electric & Autonomous Vehicles ETFs Fund of FundArmstrong CapitalNoch keine Bewertungen
- 04 - LoEPP LVM Summary Grid November 2023Dokument2 Seiten04 - LoEPP LVM Summary Grid November 2023Bati BotNoch keine Bewertungen
- Chlamydia SlidesDokument63 SeitenChlamydia Slideslia primasari100% (1)
- Full Download Book Edible Mushrooms Chemical Composition and Nutritional Value PDFDokument41 SeitenFull Download Book Edible Mushrooms Chemical Composition and Nutritional Value PDFrobert.stinson947100% (16)
- Foodlog Date 2 6 - Daily Intake 1Dokument1 SeiteFoodlog Date 2 6 - Daily Intake 1api-733085568Noch keine Bewertungen
- Properties of Common Liquids Solids and Foods 2Dokument2 SeitenProperties of Common Liquids Solids and Foods 2Šhëënà de LeonNoch keine Bewertungen
- Template02 30Dokument20 SeitenTemplate02 30sugeng abiyonoNoch keine Bewertungen
- EBLSL Daily Market Update 6th August 2020Dokument1 SeiteEBLSL Daily Market Update 6th August 2020Moheuddin SehabNoch keine Bewertungen
- The Feed Specifications Are As Follows: Table 2.4.2 Design Feed SpecificationsDokument1 SeiteThe Feed Specifications Are As Follows: Table 2.4.2 Design Feed SpecificationsRitesh Dev MaityNoch keine Bewertungen
- 02 2018 Power Statistics As of 29 March 2019 Capacity Per Plant TypeDokument2 Seiten02 2018 Power Statistics As of 29 March 2019 Capacity Per Plant TypeDominic SantiagoNoch keine Bewertungen
- BLACKCURRANT LEAF RL AllergensDokument1 SeiteBLACKCURRANT LEAF RL Allergensxxbjxkj5gjNoch keine Bewertungen
- Problem (ANOVA) : To Be Submitted/sent Until January 23, 2021Dokument1 SeiteProblem (ANOVA) : To Be Submitted/sent Until January 23, 2021JM MaguigadNoch keine Bewertungen
- Limited Asam Amino Thurain PunyaDokument1 SeiteLimited Asam Amino Thurain PunyaThurain LeoNoch keine Bewertungen
- Behavioral IntntionDokument3 SeitenBehavioral IntntionENHYPEN JAYNoch keine Bewertungen
- Book 2Dokument30 SeitenBook 2Shyam AroraNoch keine Bewertungen
- Portflio 2Dokument51 SeitenPortflio 2gurudev21Noch keine Bewertungen
- Stability Constants of Various - Thomas E. FuriaDokument12 SeitenStability Constants of Various - Thomas E. FuriaARTURONoch keine Bewertungen
- Food Log - 02-08Dokument1 SeiteFood Log - 02-08api-542235439Noch keine Bewertungen
- Balance Sheet AnalysisDokument2 SeitenBalance Sheet AnalysisAishaNoch keine Bewertungen
- Foodlog - 02 05 2024Dokument1 SeiteFoodlog - 02 05 2024api-731983167Noch keine Bewertungen
- Sodium Iodide I 131 Capsule and SolutionDokument14 SeitenSodium Iodide I 131 Capsule and SolutionPham Thanh MinhNoch keine Bewertungen
- Foodlog Date 2 3 24 - Daily IntakeDokument1 SeiteFoodlog Date 2 3 24 - Daily Intakeapi-732753029Noch keine Bewertungen
- EBLSL Daily Market Update 4th August 2020Dokument1 SeiteEBLSL Daily Market Update 4th August 2020Moheuddin SehabNoch keine Bewertungen
- Case History: BJ Chemical Services' Fastbreak in Refiner'S Test Run DataDokument2 SeitenCase History: BJ Chemical Services' Fastbreak in Refiner'S Test Run DatamacielNoch keine Bewertungen
- Refinery Air Emission MetricsDokument36 SeitenRefinery Air Emission MetricsSathish KumarNoch keine Bewertungen
- Grade 80 Lifting Chain EN818-2Dokument1 SeiteGrade 80 Lifting Chain EN818-2Kitson RolinNoch keine Bewertungen
- Energy Geopolitics by EconomidesDokument31 SeitenEnergy Geopolitics by Economidesapi-5287144Noch keine Bewertungen
- Seleccion 2 Modelos CAEXDokument3 SeitenSeleccion 2 Modelos CAEXingenieromantencionNoch keine Bewertungen
- What Is ERP: An Introduction To ERPDokument9 SeitenWhat Is ERP: An Introduction To ERPAmit AgarwalNoch keine Bewertungen
- Nutritional Composition: Values From 2003-2004 Feedstuffs Ingredient Analysis Table: Nick M. Dale and Amy B. BatalDokument2 SeitenNutritional Composition: Values From 2003-2004 Feedstuffs Ingredient Analysis Table: Nick M. Dale and Amy B. Batalasole azoxNoch keine Bewertungen
- Particulars CMP Purchase Price Purchase Value Current Value Return (%) Purchase Weightage (%) Current No of Shares Current Weightage (%)Dokument31 SeitenParticulars CMP Purchase Price Purchase Value Current Value Return (%) Purchase Weightage (%) Current No of Shares Current Weightage (%)gurudev21Noch keine Bewertungen
- Concentration Dependence of Viscosity of Alcohol Aqueous SolutionDokument5 SeitenConcentration Dependence of Viscosity of Alcohol Aqueous Solutionx0986558023Noch keine Bewertungen
- Heriot-Watt University Malaysia CampusDokument5 SeitenHeriot-Watt University Malaysia CampusAsilahNoch keine Bewertungen
- Foodlog Date 1 31 2022 - Daily IntakeDokument1 SeiteFoodlog Date 1 31 2022 - Daily Intakeapi-594256935Noch keine Bewertungen
- 1 LBNL Contributions 309.2 5,228.0 435.5 744.7 176.0 920.7 25% 232.8 1,153.4Dokument1 Seite1 LBNL Contributions 309.2 5,228.0 435.5 744.7 176.0 920.7 25% 232.8 1,153.4Akil PrabhuNoch keine Bewertungen
- ReadmeDokument67 SeitenReadmemagdalena andrewsNoch keine Bewertungen
- Exam Paper Style Samples - ChemistryDokument4 SeitenExam Paper Style Samples - ChemistryFaiz KhanNoch keine Bewertungen
- Stocks Inside Feb 2024Dokument3 SeitenStocks Inside Feb 2024dwk6q9zq25Noch keine Bewertungen
- Investment Outlook Amid Market Volatility: Amonthep Chawla, PH.DDokument16 SeitenInvestment Outlook Amid Market Volatility: Amonthep Chawla, PH.DKORNSUPA S.Noch keine Bewertungen
- BSB123 Assessment Item 2Dokument6 SeitenBSB123 Assessment Item 2Suraj ShroffNoch keine Bewertungen
- Suppliments 2Dokument2 SeitenSuppliments 2Gayathiri GovindarajuNoch keine Bewertungen
- UNIT IV - Animal NutritionDokument84 SeitenUNIT IV - Animal NutritionAngelica AgaNoch keine Bewertungen
- Leading and Lagging Strand NotesDokument3 SeitenLeading and Lagging Strand NotesAmiera AmaniNoch keine Bewertungen
- Protein Structure and FunctionDokument57 SeitenProtein Structure and FunctionZeeshan ShamimNoch keine Bewertungen
- Cell Membrane Structure and FunctionDokument21 SeitenCell Membrane Structure and FunctionPrincess Rona Velasquez AlcantaraNoch keine Bewertungen
- Amoeba Sisters Video Companion For How To Read A Codon ChartDokument2 SeitenAmoeba Sisters Video Companion For How To Read A Codon ChartThảo VânNoch keine Bewertungen
- A Simple Method For Displaying The Hydropathic Character of A ProteinDokument28 SeitenA Simple Method For Displaying The Hydropathic Character of A ProteinBiosynthesisNoch keine Bewertungen
- 8.1 Fats Carns and ProteinsDokument32 Seiten8.1 Fats Carns and ProteinsGabriel ParksNoch keine Bewertungen
- St. Viator Bilingual International School Academic Planning, Development and Assessment Code Versio DateDokument2 SeitenSt. Viator Bilingual International School Academic Planning, Development and Assessment Code Versio DateSamuel PinzonNoch keine Bewertungen
- Chapter 21 Lipid Biosynthesis (4pp) PDFDokument8 SeitenChapter 21 Lipid Biosynthesis (4pp) PDFAfdal AdhaNoch keine Bewertungen
- MWC ModelDokument2 SeitenMWC Modelrajwill1Noch keine Bewertungen
- J Efsa 2012 2557Dokument66 SeitenJ Efsa 2012 2557Diego Vazquez GomezNoch keine Bewertungen
- Option B - BiochemistryDokument24 SeitenOption B - BiochemistryRosaNoch keine Bewertungen
- DNA Structure - PowerpointDokument29 SeitenDNA Structure - PowerpointJohn Osborne100% (1)
- Replikasi, Transkripsi Dan Translasi DnaDokument19 SeitenReplikasi, Transkripsi Dan Translasi DnaEllizabeth LilantiNoch keine Bewertungen
- 363-Article Text-2752-1-10-20200430Dokument7 Seiten363-Article Text-2752-1-10-20200430ridaNoch keine Bewertungen
- Biomolecules Question Bank (Subjective)Dokument10 SeitenBiomolecules Question Bank (Subjective)Rajendra SahaNoch keine Bewertungen
- Amino Acid CatabolismDokument7 SeitenAmino Acid CatabolismAhmed Ali Mohammed AlbashirNoch keine Bewertungen
- DNA - The Double Helix - Coloring WorksheetDokument4 SeitenDNA - The Double Helix - Coloring WorksheetANGEL GUZMAN HERNANDEZNoch keine Bewertungen
- ProteinDokument8 SeitenProteinNITIN YADAVNoch keine Bewertungen
- Chapter 3 - FatsDokument4 SeitenChapter 3 - FatsSarah Demetrio NascimentoNoch keine Bewertungen
- Cell Membranes Questions - MarkschemeDokument3 SeitenCell Membranes Questions - MarkschemeDharmendra Singh50% (2)
- Dr. Marhaen Hardjo, M.Biomed, PHD: Bagian Biokimia Fakultas Kedokteran Universitas Hasanuddin MakassarDokument63 SeitenDr. Marhaen Hardjo, M.Biomed, PHD: Bagian Biokimia Fakultas Kedokteran Universitas Hasanuddin MakassarAn iNoch keine Bewertungen
- Dna Vs Rna and Protein Synthesis Updated Recap by Amoeba SistersDokument2 SeitenDna Vs Rna and Protein Synthesis Updated Recap by Amoeba SistersJaneNoch keine Bewertungen
- Multiple Choice On Proteins - MCQ Biology - Learning Biology Through MCQsDokument5 SeitenMultiple Choice On Proteins - MCQ Biology - Learning Biology Through MCQsCésar Antonio Antonio RodriguezNoch keine Bewertungen
- G10 Q4 Week3finalDokument13 SeitenG10 Q4 Week3finalANALYN DEL CASTILLONoch keine Bewertungen
- Genetic Memory PDFDokument5 SeitenGenetic Memory PDFraba100Noch keine Bewertungen
- NucleotidesDokument18 SeitenNucleotidesEmm NomanNoch keine Bewertungen
- Metabolic Biochemistry: BIBC 102Dokument38 SeitenMetabolic Biochemistry: BIBC 102FlowerNoch keine Bewertungen
- ცხიმები და ფიზიკური დატვირთვაDokument11 Seitenცხიმები და ფიზიკური დატვირთვაTinatini KurtanidzeNoch keine Bewertungen