Das könnte Ihnen auch gefallen
- NRN 202 Concept Map Patho-Altered Mental StatusDokument1 SeiteNRN 202 Concept Map Patho-Altered Mental StatusWendy Gilbert50% (2)
- Approach To Altered Mental StatusDokument19 SeitenApproach To Altered Mental StatusMudassar SattarNoch keine Bewertungen
- Cerebral Toxoplasmosis in HIV AIDS Patient: Case ReportDokument72 SeitenCerebral Toxoplasmosis in HIV AIDS Patient: Case Reportnovy rosalia chandra100% (1)
- Neurological Examination Form of Michael Sir PDFDokument27 SeitenNeurological Examination Form of Michael Sir PDFShikha Namdev100% (2)
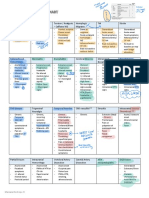
- Disease Comparison ChartDokument36 SeitenDisease Comparison ChartSara S. CastañedaNoch keine Bewertungen
- Altered Mental StateDokument2 SeitenAltered Mental Stateizzati94Noch keine Bewertungen
- Primary Headache in Clinical PracticeDokument68 SeitenPrimary Headache in Clinical PracticeAkbar RasyidsonyNoch keine Bewertungen
- Dr. Hadi Widjaja, Mbiomed, Sps Neurologist - Siloam Hospital KupangDokument23 SeitenDr. Hadi Widjaja, Mbiomed, Sps Neurologist - Siloam Hospital KupangChrysthien MarumataNoch keine Bewertungen
- 10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SDokument21 Seiten10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SSaski salsaaNoch keine Bewertungen
- Ten Tips On FeverDokument4 SeitenTen Tips On FeverOscar F RojasNoch keine Bewertungen
- 1n2 OrganicSD-drshakyaDokument26 Seiten1n2 OrganicSD-drshakyaUMESH KANDELNoch keine Bewertungen
- EpilepsyDokument37 SeitenEpilepsyMakojoa KatisoNoch keine Bewertungen
- Headache: Setyawati Asih PutriDokument79 SeitenHeadache: Setyawati Asih PutriAngga FirmansyahNoch keine Bewertungen
- Risk For IneffectiveDokument6 SeitenRisk For IneffectiveAce FabrigasNoch keine Bewertungen
- EpilepsyDokument38 SeitenEpilepsyB AuNoch keine Bewertungen
- Cerebral Palsy Nursing ManagementDokument25 SeitenCerebral Palsy Nursing ManagementpotchistroberriNoch keine Bewertungen
- Subarachnoid HemorrhageDokument2 SeitenSubarachnoid Hemorrhagevfsqp9zxgqNoch keine Bewertungen
- Epilepsy and Seizure DisordersDokument38 SeitenEpilepsy and Seizure DisordersMalueth AnguiNoch keine Bewertungen
- Paediatrics Epileptiform DisordersDokument11 SeitenPaediatrics Epileptiform DisordersayunisallehNoch keine Bewertungen
- Chronic Headache: DR Maziah BT Ishak DR Sharifah Amirah BT Syed Abd - HamidDokument30 SeitenChronic Headache: DR Maziah BT Ishak DR Sharifah Amirah BT Syed Abd - HamidSueNoch keine Bewertungen
- 10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SDokument21 Seiten10-10-2017 Sindroma Delirium Neuro. DR Hadi SP.SSaski salsaaNoch keine Bewertungen
- Migraine 2Dokument23 SeitenMigraine 2danish sultanNoch keine Bewertungen
- Module 2 - Acute Non Traumatic WeaknessDokument55 SeitenModule 2 - Acute Non Traumatic WeaknessRick RanitNoch keine Bewertungen
- Where Is The LesionDokument9 SeitenWhere Is The LesionJun 27Noch keine Bewertungen
- Nyeri Kepala 2020Dokument92 SeitenNyeri Kepala 2020Natasya Ayusandra MahersaputriNoch keine Bewertungen
- Marc Leone Ten Tips On Fever 2023Dokument4 SeitenMarc Leone Ten Tips On Fever 2023aleifelNoch keine Bewertungen
- Drug Study 1-25Dokument52 SeitenDrug Study 1-25WemslaiNoch keine Bewertungen
- Pediatric Neurology BAUDokument56 SeitenPediatric Neurology BAUمجاهد أسعدNoch keine Bewertungen
- QuizletDokument118 SeitenQuizletnaimNoch keine Bewertungen
- 2n2 OrganicSD-drshakyaDokument20 Seiten2n2 OrganicSD-drshakyaUMESH KANDELNoch keine Bewertungen
- Pid 1 86Dokument9 SeitenPid 1 86SandraNoch keine Bewertungen
- Seizures and Epilepsy in ChildhoodDokument28 SeitenSeizures and Epilepsy in Childhoodhgp9ms5gjcNoch keine Bewertungen
- Neurobiologic Theories and PsychopharmacologyDokument7 SeitenNeurobiologic Theories and PsychopharmacologyhoneyNoch keine Bewertungen
- Peripheral Neuropathy AidaDokument36 SeitenPeripheral Neuropathy AidaAdlina ArifinNoch keine Bewertungen
- Neurological Assessment - Romeo RiveraDokument9 SeitenNeurological Assessment - Romeo Riveraromeo riveraNoch keine Bewertungen
- 8) Delirium and AMS - dc.9.2.16Dokument54 Seiten8) Delirium and AMS - dc.9.2.16Jade LoberianoNoch keine Bewertungen
- Approach To Evaluation of CNS CasesDokument4 SeitenApproach To Evaluation of CNS CasesRishi ShresthaNoch keine Bewertungen
- 4 EpilepsyDokument25 Seiten4 EpilepsymuhammadridhwanNoch keine Bewertungen
- Principles of Seizure ManagementDokument119 SeitenPrinciples of Seizure ManagementRenan Toledo SandaloNoch keine Bewertungen
- Seizure and EpilepsyDokument18 SeitenSeizure and EpilepsyJamal JosephNoch keine Bewertungen
- The Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis UniversityDokument53 SeitenThe Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis Universitymonica ortizNoch keine Bewertungen
- Diagnosis Dan Klasifikasi EpilepsiDokument33 SeitenDiagnosis Dan Klasifikasi EpilepsiVhera MoksinNoch keine Bewertungen
- UntitledDokument28 SeitenUntitledAbdalla esayedNoch keine Bewertungen
- Neuropathic Pain English ClassDokument38 SeitenNeuropathic Pain English Classmulyaok285Noch keine Bewertungen
- HeadacheDokument4 SeitenHeadachejaffar mahNoch keine Bewertungen
- Head Injury TLSDokument51 SeitenHead Injury TLSNay SoeNoch keine Bewertungen
- Chapter 1Dokument182 SeitenChapter 1muntahaNoch keine Bewertungen
- Neurological AssessmentDokument43 SeitenNeurological AssessmentBhoransh VatsNoch keine Bewertungen
- Diagnoses and Management Acute Headache Emergency DepartmentDokument37 SeitenDiagnoses and Management Acute Headache Emergency DepartmentBendy Dwi IrawanNoch keine Bewertungen
- SeizuresDokument33 SeitenSeizuresLubinda SitaliNoch keine Bewertungen
- Diabetic Peripheral Neuropathic Pain (DPNP)Dokument11 SeitenDiabetic Peripheral Neuropathic Pain (DPNP)gjgibson2784Noch keine Bewertungen
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaDokument106 SeitenDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12Noch keine Bewertungen
- Neurological Coma: Zainuddin Arpandy, SP.S Neurology Department of Ulin Hospital BanjarmasinDokument24 SeitenNeurological Coma: Zainuddin Arpandy, SP.S Neurology Department of Ulin Hospital BanjarmasinDwi Rezky AmaliaNoch keine Bewertungen
- NEUROLOGY BasicsDokument179 SeitenNEUROLOGY BasicsmuntahaNoch keine Bewertungen
- Syncope PenangananDokument22 SeitenSyncope PenangananAnita PrastiwiNoch keine Bewertungen
- Management of Epilepsy: by Ejuu Seth MBCHB - 5 Facilitated by Dr. Daman AliDokument42 SeitenManagement of Epilepsy: by Ejuu Seth MBCHB - 5 Facilitated by Dr. Daman AliNinaNoch keine Bewertungen
- Neurology in TableDokument93 SeitenNeurology in TableHassan Bani SaeidNoch keine Bewertungen
- CollapseDokument46 SeitenCollapseChananNoch keine Bewertungen
- Fundamentals and Clinics of Deep Brain Stimulation: An Interdisciplinary ApproachVon EverandFundamentals and Clinics of Deep Brain Stimulation: An Interdisciplinary ApproachYasin TemelNoch keine Bewertungen
- Neurophysiology of the Migraine BrainVon EverandNeurophysiology of the Migraine BrainGianluca CoppolaNoch keine Bewertungen
- The Recent History of AcupunctureDokument2 SeitenThe Recent History of AcupunctureBhaskaranNoch keine Bewertungen
- BffsDokument60 SeitenBffsdrewantaNoch keine Bewertungen
- Lung Nodules Assessment - Analysis of Four GuidelinesDokument9 SeitenLung Nodules Assessment - Analysis of Four GuidelinesdonaskNoch keine Bewertungen
- Kodak 3D 電腦斷層系統Dokument28 SeitenKodak 3D 電腦斷層系統fomed_twNoch keine Bewertungen
- 41 - Type of Shock PDFDokument2 Seiten41 - Type of Shock PDFjamesNoch keine Bewertungen
- Nursing Care Plan-1 Age: 50Y Medical Diagnoses: Leukemia Assessment Nursing Diagnosis Planning Intervention Scientific Rationale EvaluationDokument1 SeiteNursing Care Plan-1 Age: 50Y Medical Diagnoses: Leukemia Assessment Nursing Diagnosis Planning Intervention Scientific Rationale EvaluationBheru LalNoch keine Bewertungen
- Full Book PDFDokument207 SeitenFull Book PDFsrinivasanNoch keine Bewertungen
- S: "Masakit Ang Ulo at Tiyan Niya" As Verbalized byDokument2 SeitenS: "Masakit Ang Ulo at Tiyan Niya" As Verbalized bydenise-iceNoch keine Bewertungen
- Kristal Jade Y. Esquillo: Personal DataDokument3 SeitenKristal Jade Y. Esquillo: Personal DataChristian EsquilloNoch keine Bewertungen
- Acute PancreatitisDokument7 SeitenAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- Cardiac Surgery in The Adult - 1-23Dokument23 SeitenCardiac Surgery in The Adult - 1-23Nicola AlkhorayNoch keine Bewertungen
- Diabetic FootDokument46 SeitenDiabetic FootRhapsody RedNoch keine Bewertungen
- Viral HepatitisDokument17 SeitenViral HepatitisPRATIK SHRESTHANoch keine Bewertungen
- Self Assessment Guide Pharmacy Services NC IIIDokument6 SeitenSelf Assessment Guide Pharmacy Services NC IIIAnesa TuñacaoNoch keine Bewertungen
- Family Planning MethodDokument4 SeitenFamily Planning MethodJohn Patrick G. GuevarraNoch keine Bewertungen
- PHD Thesis Hiv AidsDokument8 SeitenPHD Thesis Hiv Aidsrqopqlvcf100% (1)
- Jurnal B.inggris Kanker Prostat PDFDokument17 SeitenJurnal B.inggris Kanker Prostat PDFBoni Mohammad SalehNoch keine Bewertungen
- HealthDokument6 SeitenHealthДария КоваленкоNoch keine Bewertungen
- Pamphlet Vasectomy November 2013Dokument2 SeitenPamphlet Vasectomy November 2013KevinJanCelestinoNoch keine Bewertungen
- Work Environment, Spiritual, and Motivational Factors Affecting Job Satisfaction Among Hospital Nurses: A Systematic ReviewDokument4 SeitenWork Environment, Spiritual, and Motivational Factors Affecting Job Satisfaction Among Hospital Nurses: A Systematic ReviewMahmud Ady YuwantoNoch keine Bewertungen
- Daily Ward AssignmentsDokument4 SeitenDaily Ward AssignmentsMia Labrador Sta CruzNoch keine Bewertungen
- RCT - Masters - 2022Dokument24 SeitenRCT - Masters - 2022Kanwal KhanNoch keine Bewertungen
- I. LearningsDokument5 SeitenI. LearningsMarie Kelsey Acena MacaraigNoch keine Bewertungen
- Depression Discussion PaperDokument14 SeitenDepression Discussion Paperpinky giradoNoch keine Bewertungen
- CHARM Alt TrialDokument5 SeitenCHARM Alt TrialCristian Villarroel SNoch keine Bewertungen
- Uncoordinated ContractionsDokument23 SeitenUncoordinated ContractionsjoyceexallowNoch keine Bewertungen
- Southern Luzon State University College of Allied MedicineDokument5 SeitenSouthern Luzon State University College of Allied MedicineDan HizonNoch keine Bewertungen
- ĐỀ 24Dokument5 SeitenĐỀ 24Trang Phạm ThuNoch keine Bewertungen
- Genetic Counseling Day 2Dokument14 SeitenGenetic Counseling Day 2api-226642446Noch keine Bewertungen
- Sistem Pengurusan Kualiti: Jadual Pengajaran TerperinciDokument3 SeitenSistem Pengurusan Kualiti: Jadual Pengajaran TerperinciNurul IrhamnaNoch keine Bewertungen