Das könnte Ihnen auch gefallen
- Medical Examination Report (Aidil Fit)Dokument2 SeitenMedical Examination Report (Aidil Fit)Husni WahyudiNoch keine Bewertungen
- Off Off Off Off Off Off Off OffDokument1 SeiteOff Off Off Off Off Off Off OffHusni WahyudiNoch keine Bewertungen
- Medical Examination Report (Marginda)Dokument2 SeitenMedical Examination Report (Marginda)Husni WahyudiNoch keine Bewertungen
- Jam Kedatangan Dokter Periode 26 Okt - 25 Nop 2013Dokument29 SeitenJam Kedatangan Dokter Periode 26 Okt - 25 Nop 2013Husni WahyudiNoch keine Bewertungen
- Paket Check Up 2013Dokument5 SeitenPaket Check Up 2013Husni WahyudiNoch keine Bewertungen
- Tarif Pemeriksaan Laboratorium 2014Dokument14 SeitenTarif Pemeriksaan Laboratorium 2014Husni WahyudiNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Performance AnalyticsDokument193 SeitenPerformance AnalyticsGNoch keine Bewertungen
- CaseLaw RundownDokument1 SeiteCaseLaw RundownTrent WallaceNoch keine Bewertungen
- Paroles by PrevertDokument29 SeitenParoles by PrevertCity Lights90% (10)
- Karrnathi Undead P2Dokument2 SeitenKarrnathi Undead P2Monjis MonjasNoch keine Bewertungen
- Ptfe ManufacturingDokument16 SeitenPtfe ManufacturingKokki Kumar Dpce100% (1)
- 08 03 Runge-Kutta 2nd Order MethodDokument11 Seiten08 03 Runge-Kutta 2nd Order MethodJohn Bofarull GuixNoch keine Bewertungen
- Predictor Corrector MethodsDokument5 SeitenPredictor Corrector MethodsM2C7r6Noch keine Bewertungen
- Sample Legal Advice Problems and AnswersDokument4 SeitenSample Legal Advice Problems and AnswersJake Bryson DancelNoch keine Bewertungen
- Silk Road ActivityDokument18 SeitenSilk Road Activityapi-332313139Noch keine Bewertungen
- Seng2011 - Assignment 5Dokument11 SeitenSeng2011 - Assignment 5yajnas1996Noch keine Bewertungen
- LESSON 1 Overview of Toeic Speaking WritingDokument29 SeitenLESSON 1 Overview of Toeic Speaking WritingPhạm Thị HuyềnNoch keine Bewertungen
- ESMOE-EOST: Birth at HomeDokument4 SeitenESMOE-EOST: Birth at HomeSlindy Noty MtetwaNoch keine Bewertungen
- Commerce and Peace 11Dokument28 SeitenCommerce and Peace 11FEDERICO ORSININoch keine Bewertungen
- Gripped by The Mystery: Franziska Carolina Rehbein SspsDokument70 SeitenGripped by The Mystery: Franziska Carolina Rehbein SspsdonteldontelNoch keine Bewertungen
- Product and Services: Karmic Nakshatras in Tamil AstrologyDokument4 SeitenProduct and Services: Karmic Nakshatras in Tamil AstrologySushant ChhotrayNoch keine Bewertungen
- Talking About Special Occasions American English StudentDokument5 SeitenTalking About Special Occasions American English Studentmarinewuser8Noch keine Bewertungen
- Sacred Books of The East Series, Volume 47: Pahlavi Texts, Part FiveDokument334 SeitenSacred Books of The East Series, Volume 47: Pahlavi Texts, Part FiveJimmy T.100% (1)
- Product Manual 85018V2 (Revision F) : 505E Digital Governor For Extraction Steam TurbinesDokument160 SeitenProduct Manual 85018V2 (Revision F) : 505E Digital Governor For Extraction Steam Turbinesrahilshah100Noch keine Bewertungen
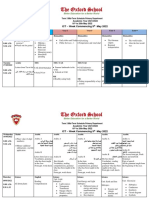
- Term 3 Mid-Term Assessment ScheduleDokument9 SeitenTerm 3 Mid-Term Assessment ScheduleRabia MoeedNoch keine Bewertungen
- EJ1266040Dokument11 SeitenEJ1266040John Lester CalleNoch keine Bewertungen
- Dina Iordanova - Women in Balkan Cinema, Surviving On The MarginsDokument17 SeitenDina Iordanova - Women in Balkan Cinema, Surviving On The MarginsimparatulverdeNoch keine Bewertungen
- Cost Accounting and Management Essentials You Always Wanted To Know: 4th EditionDokument21 SeitenCost Accounting and Management Essentials You Always Wanted To Know: 4th EditionVibrant Publishers100% (1)
- Case Theory BigamyDokument6 SeitenCase Theory BigamyLouem GarceniegoNoch keine Bewertungen
- Karling Aguilera-Fort ResumeDokument4 SeitenKarling Aguilera-Fort Resumeapi-3198760590% (1)
- Survey of World HistoryDokument77 SeitenSurvey of World Historyrufinus ondiekiNoch keine Bewertungen
- Spa IpoDokument2 SeitenSpa IpoJeff E. DatingalingNoch keine Bewertungen
- DerbyDB and EclipseDokument15 SeitenDerbyDB and EclipseHessa Al-AwwadNoch keine Bewertungen
- 00 FA17 ENG 2070 SyllabusDokument9 Seiten00 FA17 ENG 2070 SyllabusLauren SalisburyNoch keine Bewertungen
- Daad-Courses-2019-09-08 6Dokument91 SeitenDaad-Courses-2019-09-08 6Kaushik RajNoch keine Bewertungen
- PM Plan Template For PresentationDokument3 SeitenPM Plan Template For Presentationjamal123456Noch keine Bewertungen