Das könnte Ihnen auch gefallen
- Withholding and Withdrawing Life-prolonging Medical Treatment: Guidance for Decision MakingVon EverandWithholding and Withdrawing Life-prolonging Medical Treatment: Guidance for Decision MakingNoch keine Bewertungen
- World HealthDokument349 SeitenWorld HealthKo ReaNoch keine Bewertungen
- Framework For Ensuring Human Rights in The Provision of Contraceptive Information and ServicesDokument24 SeitenFramework For Ensuring Human Rights in The Provision of Contraceptive Information and ServicesSara Fernandez RiveraNoch keine Bewertungen
- Paediatric Death Audit - 9789241515184-EngDokument68 SeitenPaediatric Death Audit - 9789241515184-EngDennyNoch keine Bewertungen
- Maternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationDokument140 SeitenMaternal and Perinatal Death Surveillance and Response:: Materials To Support ImplementationBianca Maria PricopNoch keine Bewertungen
- Towards A Grand Convergence For Child Survival and HealthDokument78 SeitenTowards A Grand Convergence For Child Survival and HealthNicholasNoch keine Bewertungen
- WHO MCA 17.09 Eng PDFDokument44 SeitenWHO MCA 17.09 Eng PDFTHONDYNALUNoch keine Bewertungen
- Defeating Meningitis by 2030: A Global Road MapDokument32 SeitenDefeating Meningitis by 2030: A Global Road Mapwest.lillyNoch keine Bewertungen
- Personal Protective Equipment: For Use in A Filovirus Disease OutbreakDokument71 SeitenPersonal Protective Equipment: For Use in A Filovirus Disease Outbreakade antoNoch keine Bewertungen
- PostnatalcareguidelinesDokument73 SeitenPostnatalcareguidelinesNilakshi Barik MandalNoch keine Bewertungen
- Differentiated and Simplified Pre-Exposure Prophylaxis For HIV PreventionDokument46 SeitenDifferentiated and Simplified Pre-Exposure Prophylaxis For HIV Preventionaugusto silvaNoch keine Bewertungen
- WHO PrEP 2022Dokument48 SeitenWHO PrEP 2022OmarNoch keine Bewertungen
- Framework: For Collaborative Action On Tuberculosis and ComorbiditiesDokument88 SeitenFramework: For Collaborative Action On Tuberculosis and ComorbiditiesRatnaNoch keine Bewertungen
- Safe Abortion Care and Post-Abortion Contraception: Health Worker Roles in ProvidingDokument92 SeitenSafe Abortion Care and Post-Abortion Contraception: Health Worker Roles in Providingwelly natanael pNoch keine Bewertungen
- Maternal Health WHO 2017Dokument36 SeitenMaternal Health WHO 2017Prinnisa Almanda JonardiNoch keine Bewertungen
- WHO MCA 17.10 Eng PDFDokument36 SeitenWHO MCA 17.10 Eng PDFNia UktriaeNoch keine Bewertungen
- Meeting Expert VCM OPSDokument40 SeitenMeeting Expert VCM OPSGINA AQUINONoch keine Bewertungen
- Anc Who 2019Dokument68 SeitenAnc Who 2019Pika LubisNoch keine Bewertungen
- Who Rec For AncDokument264 SeitenWho Rec For AncBunda QueenaNoch keine Bewertungen
- Abortion Project FindingsDokument9 SeitenAbortion Project FindingsuhhmbikaNoch keine Bewertungen
- Compendium HRH Studies PDFDokument96 SeitenCompendium HRH Studies PDFkitsilcNoch keine Bewertungen
- Who Guideline AncDokument178 SeitenWho Guideline AncLina YuniartyNoch keine Bewertungen
- Who Rec For AncDokument181 SeitenWho Rec For AncDana Indania SariNoch keine Bewertungen
- INSPIRE: Seven Strategies For Ending Violence Against Children (2016)Dokument108 SeitenINSPIRE: Seven Strategies For Ending Violence Against Children (2016)Children's Institute100% (1)
- NIHRC Emergency Healthcare ReportDokument144 SeitenNIHRC Emergency Healthcare ReportCesar Roberto Braga MacedoNoch keine Bewertungen
- Standards For Improving The Quality of Care For Small and Sick Newborns in Health Facilities 2020Dokument152 SeitenStandards For Improving The Quality of Care For Small and Sick Newborns in Health Facilities 2020Shuaib KauchaliNoch keine Bewertungen
- Guidelines On HIV and Infant FeedingDokument58 SeitenGuidelines On HIV and Infant FeedingIntan AdeNoch keine Bewertungen
- WHO Guidelines For Complementary FeedingDokument96 SeitenWHO Guidelines For Complementary FeedingSiva KumarNoch keine Bewertungen
- WHO RHR 18.15 EngDokument24 SeitenWHO RHR 18.15 EngsofiabloemNoch keine Bewertungen
- COVID-19 CallDokument56 SeitenCOVID-19 CallSalve Rachelle BillenaNoch keine Bewertungen
- OMS (2011) Mhealth New HorizonsDokument112 SeitenOMS (2011) Mhealth New HorizonsFamilia Ortiz TapiaNoch keine Bewertungen
- 9789241549912-Eng (5) - DikonversiDokument172 Seiten9789241549912-Eng (5) - DikonversiAyu Sukma WulandariNoch keine Bewertungen
- 2016 WHO-CIOMS Ethical GuidelinesDokument119 Seiten2016 WHO-CIOMS Ethical Guidelinesyulianto dwi pamadiNoch keine Bewertungen
- UI Guideline - FinalDokument114 SeitenUI Guideline - FinalKrishna ChaitanyaNoch keine Bewertungen
- Communitybasedstrategiesforbreastfeedingpromotionandsupportindevelopingcountries 130209212952 Phpapp02Dokument40 SeitenCommunitybasedstrategiesforbreastfeedingpromotionandsupportindevelopingcountries 130209212952 Phpapp02JL CalvinNoch keine Bewertungen
- Iycf Who PDFDokument157 SeitenIycf Who PDFMarilyn RealistaNoch keine Bewertungen
- Consultation On: Improving Measurement of The Quality of Maternal, Newborn and Child Care in Health FacilitiesDokument43 SeitenConsultation On: Improving Measurement of The Quality of Maternal, Newborn and Child Care in Health FacilitiesKomala SariNoch keine Bewertungen
- Strategies Toward Ending Preventable Maternal Mortality (EPMM)Dokument52 SeitenStrategies Toward Ending Preventable Maternal Mortality (EPMM)Clara KarmalukNoch keine Bewertungen
- B5124Dokument91 SeitenB5124Gede JayaNoch keine Bewertungen
- Statement and Recommendations On Scaling Up HIV Testing and CounsellingDokument12 SeitenStatement and Recommendations On Scaling Up HIV Testing and CounsellingkoridoradicitaNoch keine Bewertungen
- A Global Database of Abortion Laws, Policies, Health Standards and GuidelinesDokument6 SeitenA Global Database of Abortion Laws, Policies, Health Standards and GuidelinesRahmadani NabilaNoch keine Bewertungen
- Slide Patient Safety-ADIB PDEIDokument57 SeitenSlide Patient Safety-ADIB PDEInurinkdNoch keine Bewertungen
- 609 NonDOH TelemedicineSafePerson CenteredVirtualCareDokument33 Seiten609 NonDOH TelemedicineSafePerson CenteredVirtualCarevegarciarNoch keine Bewertungen
- NHSCT/18/1216 Sterilisation GuidelineDokument8 SeitenNHSCT/18/1216 Sterilisation Guidelineana mariaNoch keine Bewertungen
- 1 - Patient Safety ConceptDokument31 Seiten1 - Patient Safety ConceptJASON KO CHIA SHENGNoch keine Bewertungen
- WHO On Tuberculosis: Operational HandbookDokument140 SeitenWHO On Tuberculosis: Operational HandbookYenny BelindaNoch keine Bewertungen
- Hannah Kuper - MB Report 2.0 - Indonesia Dec 20Dokument31 SeitenHannah Kuper - MB Report 2.0 - Indonesia Dec 20arhanNoch keine Bewertungen
- Opening Up Ethics and Disclosure en 2000Dokument43 SeitenOpening Up Ethics and Disclosure en 2000Chie CenonNoch keine Bewertungen
- Anglo TrainingGuide June2008 AdvocacyDokument123 SeitenAnglo TrainingGuide June2008 AdvocacyTse Hei Lucian ChanNoch keine Bewertungen
- WHO Study GuideDokument18 SeitenWHO Study Guidegis.kieraNoch keine Bewertungen
- WHO's Psychological Interventions Implementation ManualDokument96 SeitenWHO's Psychological Interventions Implementation ManualUtkarsh SrivastavaNoch keine Bewertungen
- Working For A Brighter, Healthier Future - How WHO Improves Health and Promotes Well-Being For The World's AdolescentsDokument70 SeitenWorking For A Brighter, Healthier Future - How WHO Improves Health and Promotes Well-Being For The World's Adolescentscosma.alina2127Noch keine Bewertungen
- Young People's Participation and Mental HealthDokument97 SeitenYoung People's Participation and Mental HealthlydomalolosNoch keine Bewertungen
- Evidence Based Obstetrics CareDokument49 SeitenEvidence Based Obstetrics CareSANANoch keine Bewertungen
- International Standards For Education of Diabetes Health ProfessionalsDokument34 SeitenInternational Standards For Education of Diabetes Health ProfessionalsCarmen UngureanuNoch keine Bewertungen
- WHO Recommendations On Drug Treatment For Non-Severe Hypertension in PregnancyDokument94 SeitenWHO Recommendations On Drug Treatment For Non-Severe Hypertension in PregnancyAshok KumarNoch keine Bewertungen
- Post Abortion Care Best Practice Paper April 2022Dokument20 SeitenPost Abortion Care Best Practice Paper April 2022Ambika dawadiNoch keine Bewertungen
- PDFDokument150 SeitenPDFLuccio RomaníNoch keine Bewertungen
- Uog 10054Dokument22 SeitenUog 10054Aswin ChristantoNoch keine Bewertungen
- Routine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolDokument15 SeitenRoutine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolYosep SutandarNoch keine Bewertungen
- Musa 2015Dokument15 SeitenMusa 2015Jose Luis Morales BautistaNoch keine Bewertungen
- PIIS000293781502102XDokument1 SeitePIIS000293781502102XYosep SutandarNoch keine Bewertungen
- Meta-Analysis of Second-Trimester Markers For Trisomy 21. 2013Dokument15 SeitenMeta-Analysis of Second-Trimester Markers For Trisomy 21. 2013risos7Noch keine Bewertungen
- Physiology of Amniotic Fluid Volume RegulationDokument8 SeitenPhysiology of Amniotic Fluid Volume RegulationYosep SutandarNoch keine Bewertungen
- Ferra RettiDokument51 SeitenFerra RettiYosep SutandarNoch keine Bewertungen
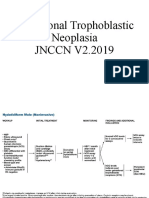
- Gestational Trophoblastic NeoplasiaDokument14 SeitenGestational Trophoblastic NeoplasiaYosep SutandarNoch keine Bewertungen
- IETADokument10 SeitenIETAJose Luis Morales BautistaNoch keine Bewertungen
- Diagnosis of Fetal Non-Chromosomal Abnormalities On Routine Ultrasound Examination at 11-13 Weeks' GestationDokument10 SeitenDiagnosis of Fetal Non-Chromosomal Abnormalities On Routine Ultrasound Examination at 11-13 Weeks' GestationYosep SutandarNoch keine Bewertungen
- Clostridium Perfringens Sepsis Following A Molar Pregnancy: ASE EportDokument2 SeitenClostridium Perfringens Sepsis Following A Molar Pregnancy: ASE EportYosep SutandarNoch keine Bewertungen
- Practice Bullet In: Emergency ContraceptionDokument11 SeitenPractice Bullet In: Emergency ContraceptionYosep SutandarNoch keine Bewertungen
- Maxillary Gap at 11-13 WeeksDokument5 SeitenMaxillary Gap at 11-13 Weekscarlos cobeloNoch keine Bewertungen
- PIIS0015028207001161Dokument8 SeitenPIIS0015028207001161Yosep SutandarNoch keine Bewertungen
- Acog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentDokument10 SeitenAcog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentYosep SutandarNoch keine Bewertungen
- PDFDokument9 SeitenPDFYosep SutandarNoch keine Bewertungen
- Pi Is 0002937817310955Dokument11 SeitenPi Is 0002937817310955Yosep SutandarNoch keine Bewertungen
- Murtagh 2010Dokument9 SeitenMurtagh 2010Yosep SutandarNoch keine Bewertungen
- Changes in The Sexual Function During Pregnancy: Aim. MethodsDokument10 SeitenChanges in The Sexual Function During Pregnancy: Aim. MethodsYosep SutandarNoch keine Bewertungen
- ISUOG - Fetal Heart ExaminationDokument12 SeitenISUOG - Fetal Heart ExaminationAzucenaNoch keine Bewertungen
- Ovarian Reserve Testing: A User's Guide: Expert ReviewsDokument12 SeitenOvarian Reserve Testing: A User's Guide: Expert ReviewsYosep SutandarNoch keine Bewertungen
- Pi Is 0884217517304100Dokument3 SeitenPi Is 0884217517304100Yosep SutandarNoch keine Bewertungen
- Effect of Pregnancy On Sexual Function of Couples: AbstractDokument8 SeitenEffect of Pregnancy On Sexual Function of Couples: AbstractYosep SutandarNoch keine Bewertungen
- Mao2014 Article ImagingOfPelvicLymphNodesDokument13 SeitenMao2014 Article ImagingOfPelvicLymphNodesYosep SutandarNoch keine Bewertungen
- Emergency Contraception: Sogc Clinical Practice GuidelineDokument9 SeitenEmergency Contraception: Sogc Clinical Practice GuidelineYosep SutandarNoch keine Bewertungen
- Systematic Reviews To Support Evidence-Based Medicine (2nd Edition)Dokument216 SeitenSystematic Reviews To Support Evidence-Based Medicine (2nd Edition)Yosep Sutandar100% (1)
- NSAMR Systematic ReviewDokument8 SeitenNSAMR Systematic ReviewYosep SutandarNoch keine Bewertungen
- Enteral NutritionDokument73 SeitenEnteral NutritionYosep SutandarNoch keine Bewertungen
- FSFI Questionnaire2000Dokument5 SeitenFSFI Questionnaire2000Dewi AsmalindaNoch keine Bewertungen
- Sikament®-4101 NS: Product Data SheetDokument2 SeitenSikament®-4101 NS: Product Data SheetShihab AhamedNoch keine Bewertungen
- Elasticity, Plasticity Structure of Matter: by DR R. HouwinkDokument9 SeitenElasticity, Plasticity Structure of Matter: by DR R. HouwinkKhlibsuwan RNoch keine Bewertungen
- Tara FeminismDokument3 SeitenTara FeminismDushyant Nimavat100% (1)
- Dental Hygienist Learning Outcomes Form v1.2Dokument32 SeitenDental Hygienist Learning Outcomes Form v1.2Karman Deep Singh100% (1)
- Make Swiss RollDokument16 SeitenMake Swiss RollFelicia LiNoch keine Bewertungen
- English CV Chis Roberta AndreeaDokument1 SeiteEnglish CV Chis Roberta AndreeaRoby ChisNoch keine Bewertungen
- Registration of Hindu Marriage: A Project On Family Law-IDokument22 SeitenRegistration of Hindu Marriage: A Project On Family Law-Iamit dipankarNoch keine Bewertungen
- Bagmati River Rejuvenation.1.0Dokument27 SeitenBagmati River Rejuvenation.1.0navonil.senNoch keine Bewertungen
- Pengaruh Skarifikasi Dan Hormon Giberelin (Ga) Terhadap Daya Kecambah Dan Pertumbuhan Bibit Palem Putri (Veitchia Merillii)Dokument8 SeitenPengaruh Skarifikasi Dan Hormon Giberelin (Ga) Terhadap Daya Kecambah Dan Pertumbuhan Bibit Palem Putri (Veitchia Merillii)Adi IndraNoch keine Bewertungen
- Normal Microflora of Human BodyDokument14 SeitenNormal Microflora of Human BodySarah PavuNoch keine Bewertungen
- Colonel SandersDokument17 SeitenColonel SandersAmandaNoch keine Bewertungen
- NANOGUARD - Products and ApplicationsDokument2 SeitenNANOGUARD - Products and ApplicationsSunrise VenturesNoch keine Bewertungen
- NG Uk RTR 0220 r15 PDFDokument9 SeitenNG Uk RTR 0220 r15 PDFDuong Thai BinhNoch keine Bewertungen
- Hand-Pallet Truck - NewDokument2 SeitenHand-Pallet Truck - NewAkhilNoch keine Bewertungen
- E GarageDokument36 SeitenE GarageLidijaSpaseskaNoch keine Bewertungen
- DiffusionDokument25 SeitenDiffusionbonginkosi mathunjwa0% (1)
- YuzurtDokument2 SeitenYuzurtFranco Ascari100% (1)
- Karan Chawla and Joshua Lee November 21, 2016 MEDS 3020 - Fall 2016 Dr. Rosevear, Dr. Cartwright, Dr. LiebermanDokument2 SeitenKaran Chawla and Joshua Lee November 21, 2016 MEDS 3020 - Fall 2016 Dr. Rosevear, Dr. Cartwright, Dr. LiebermanJeremy DelaneyNoch keine Bewertungen
- Switching Power Supply Design: A Concise Practical Handbook: February 2022Dokument5 SeitenSwitching Power Supply Design: A Concise Practical Handbook: February 2022Juan Gil RocaNoch keine Bewertungen
- of Biology On Introductory BioinformaticsDokument13 Seitenof Biology On Introductory BioinformaticsUttkarsh SharmaNoch keine Bewertungen
- FISPQ - Innova - Force - ADY - EN - 7143812336Dokument6 SeitenFISPQ - Innova - Force - ADY - EN - 7143812336Talia EllaNoch keine Bewertungen
- Standard Into-Plane Fueling Service Levels and SafetyDokument8 SeitenStandard Into-Plane Fueling Service Levels and SafetyPrekelNoch keine Bewertungen
- I. Choose The Meaning of The Underlined Words Using Context CluesDokument4 SeitenI. Choose The Meaning of The Underlined Words Using Context CluesMikko GomezNoch keine Bewertungen
- TinyEYE Online Speech Therapy Media GuideDokument4 SeitenTinyEYE Online Speech Therapy Media GuideTinyEYE Therapy ServicesNoch keine Bewertungen
- Polymer LedDokument14 SeitenPolymer LedNaveenNoch keine Bewertungen
- Steen Kamp 2021Dokument16 SeitenSteen Kamp 2021LARANSA SOLUNA GOGO SIMATUPANGNoch keine Bewertungen
- School Administration and Supervision MAED 605Dokument24 SeitenSchool Administration and Supervision MAED 605Jaynie Ann TapdasanNoch keine Bewertungen
- SCIENCE-DRRR - Q1 - W1 - Mod2Dokument16 SeitenSCIENCE-DRRR - Q1 - W1 - Mod2Jay DhelNoch keine Bewertungen
- Clack 2983 WS1EE Twin Valve LDokument2 SeitenClack 2983 WS1EE Twin Valve Lmohamed boufasNoch keine Bewertungen
- Group 4 - Cadbury - Final ProjectDokument11 SeitenGroup 4 - Cadbury - Final ProjectPravalika ReddyNoch keine Bewertungen
- Does Jesus Really Love Me?: A Gay Christian's Pilgrimage in Search of God in AmericaVon EverandDoes Jesus Really Love Me?: A Gay Christian's Pilgrimage in Search of God in AmericaBewertung: 3.5 von 5 Sternen3.5/5 (13)
- Making Gay History: The Half-Century Fight for Lesbian and Gay Equal RightsVon EverandMaking Gay History: The Half-Century Fight for Lesbian and Gay Equal RightsNoch keine Bewertungen
- Rejected Princesses: Tales of History's Boldest Heroines, Hellions, & HereticsVon EverandRejected Princesses: Tales of History's Boldest Heroines, Hellions, & HereticsBewertung: 4.5 von 5 Sternen4.5/5 (68)
- The Future Is Disabled: Prophecies, Love Notes and Mourning SongsVon EverandThe Future Is Disabled: Prophecies, Love Notes and Mourning SongsBewertung: 5 von 5 Sternen5/5 (24)
- Still Time to Care: What We Can Learn from the Church’s Failed Attempt to Cure HomosexualityVon EverandStill Time to Care: What We Can Learn from the Church’s Failed Attempt to Cure HomosexualityNoch keine Bewertungen
- Bi: The Hidden Culture, History, and Science of BisexualityVon EverandBi: The Hidden Culture, History, and Science of BisexualityBewertung: 4.5 von 5 Sternen4.5/5 (23)
- What Does the Bible Really Teach about Homosexuality?Von EverandWhat Does the Bible Really Teach about Homosexuality?Bewertung: 4.5 von 5 Sternen4.5/5 (81)
- Bending the Binary: Polarity Magic in a Non-Binary WorldVon EverandBending the Binary: Polarity Magic in a Non-Binary WorldNoch keine Bewertungen
- The Velvet Rage: Overcoming the Pain of Growing Up Gay in a Straight Man's WorldVon EverandThe Velvet Rage: Overcoming the Pain of Growing Up Gay in a Straight Man's WorldBewertung: 4.5 von 5 Sternen4.5/5 (195)
- The Marble Faun of Grey Gardens: A Memoir of the Beales, The Maysles Brothers, and Jacqueline KennedyVon EverandThe Marble Faun of Grey Gardens: A Memoir of the Beales, The Maysles Brothers, and Jacqueline KennedyBewertung: 5 von 5 Sternen5/5 (4)
- The Big Reveal: An Illustrated Manifesto of DragVon EverandThe Big Reveal: An Illustrated Manifesto of DragBewertung: 5 von 5 Sternen5/5 (14)
- Lust Unearthed: Vintage Gay Graphics From the DuBek CollectionVon EverandLust Unearthed: Vintage Gay Graphics From the DuBek CollectionBewertung: 4.5 von 5 Sternen4.5/5 (15)
- The Gay Agenda: A Modern Queer History & HandbookVon EverandThe Gay Agenda: A Modern Queer History & HandbookBewertung: 3 von 5 Sternen3/5 (9)
- UnClobber: Rethinking Our Misuse of the Bible on HomosexualityVon EverandUnClobber: Rethinking Our Misuse of the Bible on HomosexualityBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Good Boy: My Life in Seven DogsVon EverandGood Boy: My Life in Seven DogsBewertung: 3.5 von 5 Sternen3.5/5 (39)
- The Snufflington School of Online Roleplay and Basic Training for Adult pupsVon EverandThe Snufflington School of Online Roleplay and Basic Training for Adult pupsBewertung: 5 von 5 Sternen5/5 (1)
- Why Be Happy When You Could Be Normal?Von EverandWhy Be Happy When You Could Be Normal?Bewertung: 4.5 von 5 Sternen4.5/5 (11)
- Transforming: The Bible and the Lives of Transgender ChristiansVon EverandTransforming: The Bible and the Lives of Transgender ChristiansBewertung: 4.5 von 5 Sternen4.5/5 (27)
- The End of Gender: Debunking the Myths about Sex and Identity in Our SocietyVon EverandThe End of Gender: Debunking the Myths about Sex and Identity in Our SocietyBewertung: 4 von 5 Sternen4/5 (126)