Das könnte Ihnen auch gefallen
- Biotechnology in Invertebrate Pathology and Cell CultureVon EverandBiotechnology in Invertebrate Pathology and Cell CultureKarl KaramoroschNoch keine Bewertungen
- Instructions For Completing The Cause of Death Section On Death Certificate PDFDokument2 SeitenInstructions For Completing The Cause of Death Section On Death Certificate PDFpilcheritoNoch keine Bewertungen
- Blue FormDokument2 SeitenBlue Formalin_capilnean8371Noch keine Bewertungen
- Betarie Anum Almira - RMIK (A) BIK ASESMEN - IGD - PONEKDokument4 SeitenBetarie Anum Almira - RMIK (A) BIK ASESMEN - IGD - PONEKBetarie Anum AlmiraNoch keine Bewertungen
- Nursing Seminar 1 SAS Session 16Dokument8 SeitenNursing Seminar 1 SAS Session 16ZiaNoch keine Bewertungen
- Certificate - DeathDokument2 SeitenCertificate - DeathGracielle Falcasantos DalaguitNoch keine Bewertungen
- Edgcse Aap sb5 Eout High 0430Dokument7 SeitenEdgcse Aap sb5 Eout High 0430Faiar Rob Year 9Noch keine Bewertungen
- Family Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingDokument4 SeitenFamily Health Assessment Form: University of San Jose-Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNoch keine Bewertungen
- Neuropreceptorial ChecklistDokument33 SeitenNeuropreceptorial ChecklistAlloiBialba0% (1)
- 6446 PDFDokument15 Seiten6446 PDFGanesh DasaraNoch keine Bewertungen
- 11 Trauma Emergency Form 19102023Dokument2 Seiten11 Trauma Emergency Form 19102023Marjorie BricenioNoch keine Bewertungen
- Medical Law Practical Lessons 6Dokument3 SeitenMedical Law Practical Lessons 6alpanaNoch keine Bewertungen
- Medical Attendants Certificate17062019Dokument2 SeitenMedical Attendants Certificate17062019PrathameshNoch keine Bewertungen
- Annex 1Dokument3 SeitenAnnex 1Saroj PokhrelNoch keine Bewertungen
- Nursing Seminar 1 SAS Session 18Dokument8 SeitenNursing Seminar 1 SAS Session 18ZiaNoch keine Bewertungen
- Polyclinic Medical Records HistoryDokument2 SeitenPolyclinic Medical Records Historydevi ana ariesta bellaNoch keine Bewertungen
- Nursing Seminar 1 SAS Session 17Dokument8 SeitenNursing Seminar 1 SAS Session 17ZiaNoch keine Bewertungen
- Richard Missaghian, Training & Development Manager: Presented byDokument40 SeitenRichard Missaghian, Training & Development Manager: Presented byDennis GarrettNoch keine Bewertungen
- Disaster Mortality FormDokument1 SeiteDisaster Mortality FormThinaNoch keine Bewertungen
- Viral Hepatitis Case Report: Draft Copy DraftDokument6 SeitenViral Hepatitis Case Report: Draft Copy DraftMuhammad Aiman ShahzadNoch keine Bewertungen
- 07topic 7Dokument4 Seiten07topic 7noor nadhirahNoch keine Bewertungen
- MedicalDokument2 SeitenMedicalChris HutchinsonNoch keine Bewertungen
- Form 4ADokument2 SeitenForm 4Adr.bhadarkaNoch keine Bewertungen
- DiseaseSpreadSE - GizmoDokument5 SeitenDiseaseSpreadSE - GizmoSTU-Xavier GarrettNoch keine Bewertungen
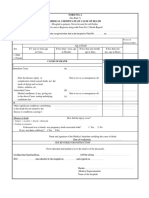
- Form No.4 (See Rule 7) Medical Certificate of Cause of DeathDokument4 SeitenForm No.4 (See Rule 7) Medical Certificate of Cause of DeathBeyza GemiciNoch keine Bewertungen
- Epilepsy Questionnaire For Proposed Insured/OwnerDokument1 SeiteEpilepsy Questionnaire For Proposed Insured/OwnerSincerely ReynNoch keine Bewertungen
- Occupational English Test Listening Test - 2Dokument6 SeitenOccupational English Test Listening Test - 2Jojelyn Yanez BaliliNoch keine Bewertungen
- 58f438da3831c - Yellow FormDokument2 Seiten58f438da3831c - Yellow FormdianaNoch keine Bewertungen
- Client Information Sheet NCM107Dokument4 SeitenClient Information Sheet NCM107Rolland Ray MendozaNoch keine Bewertungen
- Family Assessment FormDokument7 SeitenFamily Assessment Formallkhusairy6tuansiNoch keine Bewertungen
- Obstetrical History Previous Pregnancies Complicated With YES NO Family HistoryDokument2 SeitenObstetrical History Previous Pregnancies Complicated With YES NO Family HistoryDesiree Cecilio ManlangitNoch keine Bewertungen
- Medterm Ethics Comprehensive Exam BSRT 3Dokument7 SeitenMedterm Ethics Comprehensive Exam BSRT 3Lalaine De JesusNoch keine Bewertungen
- 4 MCCDForm 4Dokument2 Seiten4 MCCDForm 4Jishnu SureshNoch keine Bewertungen
- Quiz 1 NCM 112 RLEDokument3 SeitenQuiz 1 NCM 112 RLEChriz Lech50% (2)
- MRMHA C Confirmation or RevocationDokument2 SeitenMRMHA C Confirmation or RevocationprabhaNoch keine Bewertungen
- GEC Interview QuestionsDokument1 SeiteGEC Interview QuestionsTESL10621 Shameen Farah Binti Mohd AminNoch keine Bewertungen
- Pediatric Intake Form SampleDokument10 SeitenPediatric Intake Form SampleТравма ЮніверсумNoch keine Bewertungen
- Advance Referral Form 1Dokument1 SeiteAdvance Referral Form 1Khairul ScNoch keine Bewertungen
- FDA Phils-Suspected-Side-Effects-Reporting-Form-v6.0Dokument3 SeitenFDA Phils-Suspected-Side-Effects-Reporting-Form-v6.0Marizel PormilosNoch keine Bewertungen
- Nursing Seminar 1 SAS Session 4Dokument8 SeitenNursing Seminar 1 SAS Session 4ZiaNoch keine Bewertungen
- Extended Response QuestionsDokument29 SeitenExtended Response QuestionsNoor MuhammadNoch keine Bewertungen
- Nursing Seminar 1 SAS Session 2Dokument9 SeitenNursing Seminar 1 SAS Session 2ZiaNoch keine Bewertungen
- Inpatient Treatment Order - Level 2 - : (MRMHA-D)Dokument2 SeitenInpatient Treatment Order - Level 2 - : (MRMHA-D)prabhaNoch keine Bewertungen
- sb5 End of Unit Test-HigherDokument8 Seitensb5 End of Unit Test-HigherDelosh T0% (2)
- Nursing Seminar 1 SAS Session 7Dokument7 SeitenNursing Seminar 1 SAS Session 7ZiaNoch keine Bewertungen
- DA (SA) Past Papers - 2019 1st SemesterDokument77 SeitenDA (SA) Past Papers - 2019 1st SemesterYudhika NaidooNoch keine Bewertungen
- Intake Form 2020 OctDokument7 SeitenIntake Form 2020 Octapi-277069774Noch keine Bewertungen
- MRI WorksheetDokument2 SeitenMRI WorksheetDilini WijesinghNoch keine Bewertungen
- Undergraduate Nursing Program N352: Pathophysiology & Pharmacology CV Discussion Case StudyDokument7 SeitenUndergraduate Nursing Program N352: Pathophysiology & Pharmacology CV Discussion Case Studysmg267Noch keine Bewertungen
- Year 9 Biology - Unit 6 Infection and Response Mastery BookletDokument35 SeitenYear 9 Biology - Unit 6 Infection and Response Mastery BookletGabby MaeNoch keine Bewertungen
- Client Info Informed Consent To Receive Body ArtDokument2 SeitenClient Info Informed Consent To Receive Body ArtGGenZ ConsultingNoch keine Bewertungen
- Cocolife Insurance Claim 2022Dokument5 SeitenCocolife Insurance Claim 2022Shazar CarloNoch keine Bewertungen
- Medical Form For All ApplicantsDokument2 SeitenMedical Form For All ApplicantsHaason TzNoch keine Bewertungen
- Medical Abbreviations Worksheet PDFDokument2 SeitenMedical Abbreviations Worksheet PDFRupert Bautista100% (1)
- Varron - 1B - Physical Assessment FindingsDokument17 SeitenVarron - 1B - Physical Assessment FindingsDazell VarronNoch keine Bewertungen
- Guia Mitosis, Meiosis, CancerDokument6 SeitenGuia Mitosis, Meiosis, CancerManuel Sepu ArtNoch keine Bewertungen
- 5 Yrs Old BelowDokument8 Seiten5 Yrs Old BelowMarc PeraltaNoch keine Bewertungen
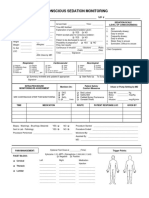
- 34 An Consious Sedation MonitoringDokument2 Seiten34 An Consious Sedation Monitoringabu alauon abed almohsenNoch keine Bewertungen
- TBDC NoDokument3 SeitenTBDC NoJohn henryNoch keine Bewertungen
- Med Info SheetDokument1 SeiteMed Info Sheetnicole5anne5ddddddNoch keine Bewertungen
- KALBO AeqweDokument2 SeitenKALBO AeqweTooter KantuterNoch keine Bewertungen
- Total Basic Annual Salary Divided by 12.: IssueDokument3 SeitenTotal Basic Annual Salary Divided by 12.: IssueTooter KantuterNoch keine Bewertungen
- Atp Compiled 1Dokument25 SeitenAtp Compiled 1Tooter KantuterNoch keine Bewertungen
- Oaminal v. CastilloDokument3 SeitenOaminal v. CastilloTooter KantuterNoch keine Bewertungen
- Petitioners Vs Vs Respondents: Third DivisionDokument7 SeitenPetitioners Vs Vs Respondents: Third DivisionTooter KantuterNoch keine Bewertungen
- Vacuo Without Reference To Attendant CircumstancesDokument4 SeitenVacuo Without Reference To Attendant CircumstancesTooter KantuterNoch keine Bewertungen
- Teodoro V ManaloDokument17 SeitenTeodoro V ManaloTooter KantuterNoch keine Bewertungen
- Inter Office MemoDokument6 SeitenInter Office MemoTooter Kantuter0% (1)
- Jaymie Jeane Gan Yu: ObjectiveDokument4 SeitenJaymie Jeane Gan Yu: ObjectiveTooter KantuterNoch keine Bewertungen
- Romualdez-Marcos v. Commission On ElectionsDokument7 SeitenRomualdez-Marcos v. Commission On ElectionsTooter KantuterNoch keine Bewertungen
- Legal Separation DigestDokument18 SeitenLegal Separation DigestTooter KantuterNoch keine Bewertungen
- Compiled Notes - Seminar Micro 1Dokument7 SeitenCompiled Notes - Seminar Micro 1Tooter KantuterNoch keine Bewertungen
- Mrrivera & AssociatesDokument2 SeitenMrrivera & AssociatesTooter KantuterNoch keine Bewertungen
- Appellants Brief Civil ScribdDokument5 SeitenAppellants Brief Civil ScribdTooter KantuterNoch keine Bewertungen
- Santillon Vs MirandaDokument1 SeiteSantillon Vs MirandaTooter KantuterNoch keine Bewertungen
- Late-August 2014 (Grade 9) St. Augustine St. Jude St. VincentDokument1 SeiteLate-August 2014 (Grade 9) St. Augustine St. Jude St. VincentTooter KantuterNoch keine Bewertungen
- COVID 19 PANDEMIC, PROFIT, FALLOUT - Harrison Research Report On Covid19Dokument229 SeitenCOVID 19 PANDEMIC, PROFIT, FALLOUT - Harrison Research Report On Covid19Peter100% (1)
- Form No.4 (See Rule 7) Medical Certificate of Cause of DeathDokument4 SeitenForm No.4 (See Rule 7) Medical Certificate of Cause of DeathBeyza GemiciNoch keine Bewertungen
- English Pre Board 1 XIIDokument12 SeitenEnglish Pre Board 1 XIIChirag BansalNoch keine Bewertungen
- Brought Dead Protocol - RefDokument2 SeitenBrought Dead Protocol - Refjesvin prathapNoch keine Bewertungen
- Medical Certification of Cause of Death: Review ArticleDokument12 SeitenMedical Certification of Cause of Death: Review Articleniraj_sdNoch keine Bewertungen
- Death Note RulesDokument10 SeitenDeath Note RulesShiraMeikoNoch keine Bewertungen
- Module 4 - Death Certification and Cause of Death - 2Dokument21 SeitenModule 4 - Death Certification and Cause of Death - 2anton_susanto10Noch keine Bewertungen
- Notes On How To Fill in The Medical Certificate of Cause of DeathDokument10 SeitenNotes On How To Fill in The Medical Certificate of Cause of DeathSayantan BanerjeeNoch keine Bewertungen
- Multnomah County's Report On Homeless Deaths in 2022Dokument28 SeitenMultnomah County's Report On Homeless Deaths in 2022KGW News100% (1)
- Certification of Cause of DeathDokument9 SeitenCertification of Cause of DeathMoses MwauraNoch keine Bewertungen
- Rules of The Death NoteDokument24 SeitenRules of The Death NoteLaknyer75% (4)
- GR 176832Dokument5 SeitenGR 176832Jhudith De Julio BuhayNoch keine Bewertungen
- DOH Administrative Order 2020-0008Dokument20 SeitenDOH Administrative Order 2020-0008qmmc.adjudicatormd100% (1)
- Michael Goss - Death CertificateDokument1 SeiteMichael Goss - Death CertificateAlex EstradaNoch keine Bewertungen
- Abdelmonem Goda Madboly - Accuracy of Medical Certification of Cause of Death AfterDokument23 SeitenAbdelmonem Goda Madboly - Accuracy of Medical Certification of Cause of Death Afterniraj_sdNoch keine Bewertungen
- Mortality CodingDokument15 SeitenMortality Codingma celine villoNoch keine Bewertungen
- Overview of New Death Certificate PDFDokument59 SeitenOverview of New Death Certificate PDFFaisol KabirNoch keine Bewertungen
- Causes of DeathDokument19 SeitenCauses of DeathramilflecoNoch keine Bewertungen
- 1.3.1 The Autopsy-1Dokument4 Seiten1.3.1 The Autopsy-1Alyssa robertsNoch keine Bewertungen
- Ambler Custodial Death ReportDokument7 SeitenAmbler Custodial Death ReportAnonymous Pb39klJ0% (1)