Das könnte Ihnen auch gefallen
- CXC - Past - Paper - 2022 Solutions PDFDokument17 SeitenCXC - Past - Paper - 2022 Solutions PDFDarren Fraser100% (1)
- Chemical Quick Guide PDFDokument1 SeiteChemical Quick Guide PDFAndrejs ZundaNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 16: HematologyVon EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNoch keine Bewertungen
- Hope Hospital Self Assessment ToolkitDokument120 SeitenHope Hospital Self Assessment Toolkitcxz4321Noch keine Bewertungen
- New Red Blood Cell and Reticulocyte Parameters and Reference Values For Healthy Individuals and in Chronic Kidney Disease.Dokument8 SeitenNew Red Blood Cell and Reticulocyte Parameters and Reference Values For Healthy Individuals and in Chronic Kidney Disease.Alberto MarcosNoch keine Bewertungen
- Appendix B - Distance Tables - Metric Units PDFDokument15 SeitenAppendix B - Distance Tables - Metric Units PDFitisINoch keine Bewertungen
- Disorders of Iron MetabolismDokument42 SeitenDisorders of Iron MetabolismFatima ZuhraNoch keine Bewertungen
- Jeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFDokument337 SeitenJeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFBruno de CastroNoch keine Bewertungen
- The Vapour Compression Cycle (Sample Problems)Dokument3 SeitenThe Vapour Compression Cycle (Sample Problems)allovid33% (3)
- Bedwetting TCMDokument5 SeitenBedwetting TCMRichonyouNoch keine Bewertungen
- Doctors ListDokument212 SeitenDoctors ListSaranya Chandrasekar33% (3)
- Reticulocyte Hemoglobin Content: Alan E. Mast, Morey A. Blinder, and Dennis J. DietzenDokument4 SeitenReticulocyte Hemoglobin Content: Alan E. Mast, Morey A. Blinder, and Dennis J. DietzenLoudry ElfaNoch keine Bewertungen
- Soluble Transferrin Receptors and Reticulocyte Hemoglobin Concentration in The Assessment in Iron Deficiency in Hemodialysis PatientsDokument9 SeitenSoluble Transferrin Receptors and Reticulocyte Hemoglobin Concentration in The Assessment in Iron Deficiency in Hemodialysis PatientsMuhammad HafidNoch keine Bewertungen
- Using The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerDokument7 SeitenUsing The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerMekar PalupiNoch keine Bewertungen
- Validation Biochemistry MeasurementDokument35 SeitenValidation Biochemistry Measurementhudan aziziNoch keine Bewertungen
- JofIMAB - 2016 22 2p1127 1131Dokument5 SeitenJofIMAB - 2016 22 2p1127 1131Oktaviana NikenNoch keine Bewertungen
- Diagnosis of Iron Deficiency of Chronic Kidney Disease: Validity OF Iron Parameters, Reticulocyte Hemoglobin Content (CHR) AND Hypochromic Red Cells in Inflammatory StateDokument9 SeitenDiagnosis of Iron Deficiency of Chronic Kidney Disease: Validity OF Iron Parameters, Reticulocyte Hemoglobin Content (CHR) AND Hypochromic Red Cells in Inflammatory StatemargaruzzaNoch keine Bewertungen
- Serum Transferrin Receptor and Transferrin Receptor-Ferritin Index Identify Healthy Subjects With Subclinical Iron DeficitsDokument6 SeitenSerum Transferrin Receptor and Transferrin Receptor-Ferritin Index Identify Healthy Subjects With Subclinical Iron DeficitsekoNoch keine Bewertungen
- Iron Overload in Beta Thalassemia PDFDokument5 SeitenIron Overload in Beta Thalassemia PDFyesikaNoch keine Bewertungen
- Alt Ast - Serum FerritinDokument10 SeitenAlt Ast - Serum FerritinMino TaeNoch keine Bewertungen
- Meta Analisis StudiDokument13 SeitenMeta Analisis StudiShafira Maulani putriNoch keine Bewertungen
- Biomedj 256 14R11Dokument15 SeitenBiomedj 256 14R11Bassem RefaatNoch keine Bewertungen
- Soluble Transferrin Receptor As A Diagnostic Laboratory Test For Detection of Iron Deficiency Anemia in Acute Illness of Hospitalized PatientsDokument3 SeitenSoluble Transferrin Receptor As A Diagnostic Laboratory Test For Detection of Iron Deficiency Anemia in Acute Illness of Hospitalized PatientsAldila VidyaNoch keine Bewertungen
- Jurnal InternasionalDokument6 SeitenJurnal Internasionalbela melizaNoch keine Bewertungen
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Dokument8 SeitenDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeNoch keine Bewertungen
- Diagnostic Accuracy of Serum Iron and Total Iron Binding Capacity (TIBC) in Iron Deficiency StateDokument4 SeitenDiagnostic Accuracy of Serum Iron and Total Iron Binding Capacity (TIBC) in Iron Deficiency StateTanveerNoch keine Bewertungen
- A572 PDFDokument4 SeitenA572 PDFTanveerNoch keine Bewertungen
- Anemia 1Dokument8 SeitenAnemia 1Patrick ValentinoNoch keine Bewertungen
- 012 Analysis of Reticulocyte Parameters On The Sysmex XEDokument8 Seiten012 Analysis of Reticulocyte Parameters On The Sysmex XEblanket_thNoch keine Bewertungen
- Saliva Iron and Ferritin Levels in PatieDokument3 SeitenSaliva Iron and Ferritin Levels in Patieالحب الابديNoch keine Bewertungen
- Low Alt CKDDokument5 SeitenLow Alt CKDFebianti RukmanaNoch keine Bewertungen
- Erythropoietic Activity and Soluble Transferrin Receptor Level in Neonates and Maternal BloodDokument5 SeitenErythropoietic Activity and Soluble Transferrin Receptor Level in Neonates and Maternal BloodDwi AryanataNoch keine Bewertungen
- Comment On Does Zinc Supplementation Affect Inflammatory Markers in Hemodialysis PatientsDokument3 SeitenComment On Does Zinc Supplementation Affect Inflammatory Markers in Hemodialysis PatientscsandrasNoch keine Bewertungen
- Investigation of The Etiology of Anemia in Thromboangiitis ObliteransDokument6 SeitenInvestigation of The Etiology of Anemia in Thromboangiitis ObliteransHusni mubarakNoch keine Bewertungen
- Intravenous Iron and Maintenance Hemodialysis: CorrespondenceDokument3 SeitenIntravenous Iron and Maintenance Hemodialysis: CorrespondenceSamanthaNoch keine Bewertungen
- Blunted Hepcidin Response To Oral Iron Challenge in HFE Related He - 2007 - BlooDokument5 SeitenBlunted Hepcidin Response To Oral Iron Challenge in HFE Related He - 2007 - BlooTareeqanwar MohammedNoch keine Bewertungen
- 154-Article Text-355-1-10-20171204Dokument8 Seiten154-Article Text-355-1-10-20171204Polyfine Nutra-SciencesNoch keine Bewertungen
- Renal Anemia Guidelines BookletDokument12 SeitenRenal Anemia Guidelines BookletDeepaNoch keine Bewertungen
- 271 592 1 SMDokument7 Seiten271 592 1 SMShandi Iriana SitorusNoch keine Bewertungen
- Articulo 2 YaDokument9 SeitenArticulo 2 YaLaura EscobarNoch keine Bewertungen
- Florit 2012Dokument3 SeitenFlorit 2012BEATRIZ CUBILLONoch keine Bewertungen
- 1-3 Meta AnalysisDokument81 Seiten1-3 Meta Analysismarryskye9Noch keine Bewertungen
- 1 s2.0 S0272638614013572 Main PDFDokument9 Seiten1 s2.0 S0272638614013572 Main PDFemyNoch keine Bewertungen
- Anemia Besi Di Pasien HFDokument14 SeitenAnemia Besi Di Pasien HFAdipNoch keine Bewertungen
- Advances in Medical SciencesDokument6 SeitenAdvances in Medical SciencesMihaela-Alexandra PopNoch keine Bewertungen
- Journal Reading Wajib GastroDokument15 SeitenJournal Reading Wajib GastroKarunia Dias BhaskoroNoch keine Bewertungen
- Main Article - BM PancytopeniaDokument10 SeitenMain Article - BM PancytopeniaAbdur Rachman Ba'abdullahNoch keine Bewertungen
- Research Paper: 10 Ml/min DecreaseDokument11 SeitenResearch Paper: 10 Ml/min DecreaseRizka Nurul FirdausNoch keine Bewertungen
- Hepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyDokument10 SeitenHepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyjNoch keine Bewertungen
- Anem 2Dokument6 SeitenAnem 2vamiqrasoolNoch keine Bewertungen
- Changes in Urine Volume and Serum Albumin in Incident Hemodialysis PatientsDokument12 SeitenChanges in Urine Volume and Serum Albumin in Incident Hemodialysis Patientsmelda lestari haidirNoch keine Bewertungen
- Journal 2Dokument3 SeitenJournal 2Anis Rita PratiwiNoch keine Bewertungen
- Retic IronDokument4 SeitenRetic IronIndahNoch keine Bewertungen
- Changes in Echocardiographic Parameters in Iron Deficiency Patients With Heart Failure and Chronic Kidney Disease Treated With Intravenous IronDokument10 SeitenChanges in Echocardiographic Parameters in Iron Deficiency Patients With Heart Failure and Chronic Kidney Disease Treated With Intravenous IronYan Hein TanawaniNoch keine Bewertungen
- Sharawey2011 PDFDokument7 SeitenSharawey2011 PDFIkram DibNoch keine Bewertungen
- Hepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyDokument17 SeitenHepcidin As A Diagnostic Biomarker of Iron Deficiency Anemia During PregnancyAgungBudiPamungkasNoch keine Bewertungen
- Reticulocyte Hemoglobin Equivalent As A Potential Marker PDFDokument10 SeitenReticulocyte Hemoglobin Equivalent As A Potential Marker PDFFrancoNoch keine Bewertungen
- Thalassemia IndiaDokument4 SeitenThalassemia IndiaDr Laxmikant Basavraj DamaNoch keine Bewertungen
- BM and Iron ProfileDokument5 SeitenBM and Iron ProfileShila SahaNoch keine Bewertungen
- Hypocalcemia Pada Beta Thalassemia PDFDokument3 SeitenHypocalcemia Pada Beta Thalassemia PDFYohana Elisabeth GultomNoch keine Bewertungen
- Lack of Clinical Utility of Folate Levels in The eDokument3 SeitenLack of Clinical Utility of Folate Levels in The eFabio Henrique PetitoNoch keine Bewertungen
- The Effects of Iron Treatment On Viscosity in Children With Cyanotic Congenital Heart DiseaseDokument7 SeitenThe Effects of Iron Treatment On Viscosity in Children With Cyanotic Congenital Heart DiseasemuhammadrikiNoch keine Bewertungen
- Thalassemia JournalDokument8 SeitenThalassemia JournalHanako AranillaNoch keine Bewertungen
- TRF PRC 1Dokument5 SeitenTRF PRC 1muhammad rezaNoch keine Bewertungen
- Anemia and Thrombocytopenia in Acute and Chronic Renal Failure PDFDokument6 SeitenAnemia and Thrombocytopenia in Acute and Chronic Renal Failure PDFSatriyo Dwi SuryantoroNoch keine Bewertungen
- Joo Sten 2017Dokument7 SeitenJoo Sten 2017langit rizki yuditamaNoch keine Bewertungen
- The Relationship Between Anemia, Liver Disease, and Hepcidin Levels in Hemodialysis Patients With HepatitisDokument4 SeitenThe Relationship Between Anemia, Liver Disease, and Hepcidin Levels in Hemodialysis Patients With HepatitisDaitya Rangga SaputraNoch keine Bewertungen
- Eritropoetin HiporesponsivDokument5 SeitenEritropoetin Hiporesponsivadri20121989Noch keine Bewertungen
- Quran Ki MarifatDokument72 SeitenQuran Ki MarifatTanveerNoch keine Bewertungen
- AyeshaDokument3 SeitenAyeshaTanveerNoch keine Bewertungen
- Ayesha Umar Wahedi - CV 2016Dokument4 SeitenAyesha Umar Wahedi - CV 2016TanveerNoch keine Bewertungen
- Ayesha KausarDokument3 SeitenAyesha KausarTanveerNoch keine Bewertungen
- Curriculum VitaeDokument4 SeitenCurriculum VitaeTanveerNoch keine Bewertungen
- Curriculum Vitae: Dr. Sartaj Alam SyedDokument8 SeitenCurriculum Vitae: Dr. Sartaj Alam SyedTanveerNoch keine Bewertungen
- Ayesha S. Mahmud: Current PositionDokument5 SeitenAyesha S. Mahmud: Current PositionTanveerNoch keine Bewertungen
- 14145527801159Dokument9 Seiten14145527801159TanveerNoch keine Bewertungen
- Shaukat Ali: Curriculum VitaeDokument8 SeitenShaukat Ali: Curriculum VitaeTanveerNoch keine Bewertungen
- DR Shaukat (Plant Pathology)Dokument5 SeitenDR Shaukat (Plant Pathology)Tanveer100% (1)
- Ali, Shaukat CV - Pubs Fy16 - 0Dokument3 SeitenAli, Shaukat CV - Pubs Fy16 - 0TanveerNoch keine Bewertungen
- Europass Curriculum Vitae: Personal Information Popescu Simona-AlinaDokument11 SeitenEuropass Curriculum Vitae: Personal Information Popescu Simona-AlinaTanveerNoch keine Bewertungen
- Resume Muhammad Asif Sadiq Deputy Registrar GC University LahoreDokument1 SeiteResume Muhammad Asif Sadiq Deputy Registrar GC University LahoreTanveer100% (1)
- CV - Gaurav BahlDokument17 SeitenCV - Gaurav BahlTanveerNoch keine Bewertungen
- Wajid CVDokument13 SeitenWajid CVTanveerNoch keine Bewertungen
- Hussain I - CV 2016 - LumsDokument8 SeitenHussain I - CV 2016 - LumsTanveerNoch keine Bewertungen
- 1359443692128Dokument10 Seiten1359443692128TanveerNoch keine Bewertungen
- Curriculum Vitae: Dr. Tayyab SubhaniDokument13 SeitenCurriculum Vitae: Dr. Tayyab SubhaniTanveerNoch keine Bewertungen
- DR Shah (New CV)Dokument7 SeitenDR Shah (New CV)TanveerNoch keine Bewertungen
- Minutes of Pre-Bid Meeting & Procurement of Consultancy Services To Conduct Feasibility Study For Establishing Monorail System Along Lahore Canal Road 17012014 0 0 2Dokument92 SeitenMinutes of Pre-Bid Meeting & Procurement of Consultancy Services To Conduct Feasibility Study For Establishing Monorail System Along Lahore Canal Road 17012014 0 0 2TanveerNoch keine Bewertungen
- CV 22 09 2018Dokument37 SeitenCV 22 09 2018TanveerNoch keine Bewertungen
- Bio Tech Shankar Ayaz AhmadDokument14 SeitenBio Tech Shankar Ayaz AhmadTanveerNoch keine Bewertungen
- Curriculum Vitae Muhammad Wajid Raza: 1.contact InformationDokument4 SeitenCurriculum Vitae Muhammad Wajid Raza: 1.contact InformationTanveer100% (1)
- Muhammad Yasir Yaqoob: ContactDokument2 SeitenMuhammad Yasir Yaqoob: ContactTanveerNoch keine Bewertungen
- Rana Rubnawaz CV - 2014Dokument2 SeitenRana Rubnawaz CV - 2014TanveerNoch keine Bewertungen
- Interneelist2013 PDFDokument40 SeitenInterneelist2013 PDFTanveerNoch keine Bewertungen
- Salaheddin R. Malkawi: Salahm@just - Edu.joDokument8 SeitenSalaheddin R. Malkawi: Salahm@just - Edu.joTanveerNoch keine Bewertungen
- DR Munir AhmadDokument12 SeitenDR Munir AhmadTanveerNoch keine Bewertungen
- Curriculum Vitae: Area of InterestDokument18 SeitenCurriculum Vitae: Area of InterestTanveerNoch keine Bewertungen
- Curriculum Vitae: Dr. Sohail AhmadDokument7 SeitenCurriculum Vitae: Dr. Sohail AhmadTanveerNoch keine Bewertungen
- SGT PDFDokument383 SeitenSGT PDFDushyanthkumar DasariNoch keine Bewertungen
- Terminologi AnatomiaDokument49 SeitenTerminologi AnatomiaLuluk QurrataNoch keine Bewertungen
- Characteristics of Testable HypothesesDokument30 SeitenCharacteristics of Testable HypothesesMarivic Diano67% (3)
- HVAC (Heating, Ventilation and Air Conditioning) : SRS PrecautionsDokument1 SeiteHVAC (Heating, Ventilation and Air Conditioning) : SRS PrecautionssoftallNoch keine Bewertungen
- Those With MoonDokument1 SeiteThose With MoonRosee AldamaNoch keine Bewertungen
- 7 UpDokument3 Seiten7 UpRajeev TripathiNoch keine Bewertungen
- 6Dokument2 Seiten6Min Hsuan HsianNoch keine Bewertungen
- REV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Dokument2 SeitenREV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Bacano CapoeiraNoch keine Bewertungen
- Dressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionDokument2 SeitenDressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionAlvaCatalinaNoch keine Bewertungen
- Organogram - Qa / QC: Srinivasan SrinivasanDokument4 SeitenOrganogram - Qa / QC: Srinivasan SrinivasanGowtham VenkatNoch keine Bewertungen
- Mil STD 792fDokument13 SeitenMil STD 792fdoradoanNoch keine Bewertungen
- Current Concepts of Enzyme Histochemistry in Modern PathologyDokument11 SeitenCurrent Concepts of Enzyme Histochemistry in Modern PathologyRosa AquinoNoch keine Bewertungen
- Pengaruh Kualitas Anc Dan Riwayat Morbiditas Maternal Terhadap Morbiditas Maternal Di Kabupaten SidoarjoDokument9 SeitenPengaruh Kualitas Anc Dan Riwayat Morbiditas Maternal Terhadap Morbiditas Maternal Di Kabupaten Sidoarjohikmah899Noch keine Bewertungen
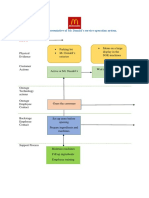
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDokument2 SeitenBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNoch keine Bewertungen
- How McDonald'sDokument2 SeitenHow McDonald'spratik khandualNoch keine Bewertungen
- Brief RESUME EmailDokument4 SeitenBrief RESUME Emailranjit_kadalg2011Noch keine Bewertungen
- Wisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseDokument3 SeitenWisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseTMJ4 NewsNoch keine Bewertungen
- IPG Or-01 - PTC Train Infrastructure Electrical Safety RulesDokument50 SeitenIPG Or-01 - PTC Train Infrastructure Electrical Safety Rules4493464Noch keine Bewertungen
- Rules For State Competitions and Iabf Approved TournamentsDokument56 SeitenRules For State Competitions and Iabf Approved TournamentsQuality management systems documentsNoch keine Bewertungen
- Uas MR1Dokument2 SeitenUas MR1IvanNoch keine Bewertungen
- G1 Series User Manual Ver. 1.2Dokument101 SeitenG1 Series User Manual Ver. 1.2unedo parhusip100% (1)
- Heteropolyacids FurfuralacetoneDokument12 SeitenHeteropolyacids FurfuralacetonecligcodiNoch keine Bewertungen