Das könnte Ihnen auch gefallen
- Endocrine Surgery: Butterworths International Medical Reviews: SurgeryVon EverandEndocrine Surgery: Butterworths International Medical Reviews: SurgeryI. D. A. JohnstonNoch keine Bewertungen
- Lavado IntraventricularDokument8 SeitenLavado IntraventricularGlessin MurilloNoch keine Bewertungen
- 2012 - Frympas G.Dokument8 Seiten2012 - Frympas G.alejandra gonzalezNoch keine Bewertungen
- 2013 - BoghaniDokument11 Seiten2013 - Boghanialejandra gonzalezNoch keine Bewertungen
- 2022 Perioperative Complications of Transvenous Embolization of Ruptured Intracranial Arteriovenous MalformationsDokument7 Seiten2022 Perioperative Complications of Transvenous Embolization of Ruptured Intracranial Arteriovenous MalformationsstaseaditNoch keine Bewertungen
- Guo 2019Dokument8 SeitenGuo 2019Dr. Gerald ToyoNoch keine Bewertungen
- Predictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageDokument8 SeitenPredictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageNovia AyuNoch keine Bewertungen
- A Case Report On Middle Cerebral Artery Aneurysm.44Dokument5 SeitenA Case Report On Middle Cerebral Artery Aneurysm.44SuNil AdhiKariNoch keine Bewertungen
- 1 s2.0 S0929664617300487 MainDokument8 Seiten1 s2.0 S0929664617300487 MainSuryati HusinNoch keine Bewertungen
- EsofagoDokument6 SeitenEsofagoWillie VanegasNoch keine Bewertungen
- Meroni2017 CompressedDokument8 SeitenMeroni2017 Compresseddayllyn iglesiasNoch keine Bewertungen
- Chirurgia Hemoragiei Din Ganglionii BazaliDokument8 SeitenChirurgia Hemoragiei Din Ganglionii BazaliAndreea DanielaNoch keine Bewertungen
- Rare and Fatal Complications of Tonsillectomy Sudden Pneumothorax and Extensive Subcutaneous EmphysemaDokument8 SeitenRare and Fatal Complications of Tonsillectomy Sudden Pneumothorax and Extensive Subcutaneous EmphysemaJoko NugrohoNoch keine Bewertungen
- AngiofibromaDokument7 SeitenAngiofibromaPandu DiputraNoch keine Bewertungen
- Primary Operative Renal Salvage of Grade-4 Blunt Renal Injury: A Case ReportDokument4 SeitenPrimary Operative Renal Salvage of Grade-4 Blunt Renal Injury: A Case ReportArsyad FadliNoch keine Bewertungen
- Ho Et Al 2022 Management of Descending Necrotizing Mediastinitis A Severe Complication of Deep Neck Infection Based OnDokument8 SeitenHo Et Al 2022 Management of Descending Necrotizing Mediastinitis A Severe Complication of Deep Neck Infection Based OncharlaayasyafefiNoch keine Bewertungen
- Middle Meningeal Artery Embolization For Chronic Subdural Hematoma in Elderly Patients at High Risk of Surgical TreatmentDokument8 SeitenMiddle Meningeal Artery Embolization For Chronic Subdural Hematoma in Elderly Patients at High Risk of Surgical TreatmentJUANNoch keine Bewertungen
- Tto VasoespasmoDokument6 SeitenTto VasoespasmoHernando CastrillónNoch keine Bewertungen
- 2 5373127936972950922Dokument6 Seiten2 5373127936972950922teguh sNoch keine Bewertungen
- Neurogenic Pulmonary Edema Due To Traumatic Brain Injury Evidence of Cardiac DysfunctionDokument10 SeitenNeurogenic Pulmonary Edema Due To Traumatic Brain Injury Evidence of Cardiac DysfunctionydtrgnNoch keine Bewertungen
- Postoperative Meningitis After Spinal Surgery: A Review of 21 Cases From 20,178 PatientsDokument5 SeitenPostoperative Meningitis After Spinal Surgery: A Review of 21 Cases From 20,178 PatientsntnquynhproNoch keine Bewertungen
- Septic PatientsDokument12 SeitenSeptic PatientsBruno NdoumouNoch keine Bewertungen
- Predictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary TumorsDokument6 SeitenPredictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary Tumorsfabian arassiNoch keine Bewertungen
- Jurnal AnastesiDokument7 SeitenJurnal AnastesiStefania MarlinaNoch keine Bewertungen
- Short - and Long-Term Outcomes at A Single InstitutionDokument7 SeitenShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahNoch keine Bewertungen
- Intraoperative Hemoadsorption in High-Risk PatientDokument13 SeitenIntraoperative Hemoadsorption in High-Risk Patientmuhammad24fayazNoch keine Bewertungen
- 2018 - Article Erdocan 8p.pdf - CopieDokument6 Seiten2018 - Article Erdocan 8p.pdf - CopieThomas HussonNoch keine Bewertungen
- Precedex Delirium Spine - AA2023Dokument9 SeitenPrecedex Delirium Spine - AA2023Ahida VelazquezNoch keine Bewertungen
- Perioperative Management of AdrenalectomyDokument13 SeitenPerioperative Management of AdrenalectomyTJ LapuzNoch keine Bewertungen
- Intracerebral and Subarachnoid Hemorrhage in Patients With CancerDokument8 SeitenIntracerebral and Subarachnoid Hemorrhage in Patients With CancerMadeNoch keine Bewertungen
- EJCO - Volume 6 - Issue 2 - Pages 117-123Dokument7 SeitenEJCO - Volume 6 - Issue 2 - Pages 117-123doaa ahmadNoch keine Bewertungen
- Epidermoid Cysts TNEDokument10 SeitenEpidermoid Cysts TNEbello_england_209552Noch keine Bewertungen
- Ich - Inducido Por DrogasDokument14 SeitenIch - Inducido Por DrogasMarceloAndresCastañedaDuarteNoch keine Bewertungen
- Avaliação Ultra-Sonográfica Das Técnicas de Punção Da Veia Jugular Interna em CriançasDokument4 SeitenAvaliação Ultra-Sonográfica Das Técnicas de Punção Da Veia Jugular Interna em CriançasJing CruzNoch keine Bewertungen
- 1 s2.0 S0104001421000385 MainDokument4 Seiten1 s2.0 S0104001421000385 MainSuci dwi CahyaNoch keine Bewertungen
- Role of Ultrasonographic Inferior Venacaval Assessment in Surgeries Conducted Under General Anaesthesia-A Prospective Observational StudyDokument6 SeitenRole of Ultrasonographic Inferior Venacaval Assessment in Surgeries Conducted Under General Anaesthesia-A Prospective Observational StudyIJAR JOURNALNoch keine Bewertungen
- Original Article: ArticleinfoDokument5 SeitenOriginal Article: ArticleinfoBIOMEDSCIDIRECT PUBLICATIONSNoch keine Bewertungen
- Topical Steroids in Rhinosinusitis and Intraoperative Bleeding: More Harm Than Good?Dokument7 SeitenTopical Steroids in Rhinosinusitis and Intraoperative Bleeding: More Harm Than Good?lala poNoch keine Bewertungen
- Juvenile Nasopharyngeal Angiofibroma - A Hospital-Based Retrospective StudyDokument3 SeitenJuvenile Nasopharyngeal Angiofibroma - A Hospital-Based Retrospective StudyGiiszs AlvarezNoch keine Bewertungen
- (10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsDokument7 Seiten(10920684 - Neurosurgical Focus) Falcotentorial Meningiomas - Clinical, Neuroimaging, and Surgical Features in Six PatientsPutri PrameswariNoch keine Bewertungen
- Diagnosis and Treatment of Pericallosal Artery Aneurysms: SciencedirectDokument4 SeitenDiagnosis and Treatment of Pericallosal Artery Aneurysms: SciencedirectRais RyuzakiNoch keine Bewertungen
- Nihms 805170Dokument16 SeitenNihms 805170Santri WelayNoch keine Bewertungen
- HEMOPTISISDokument6 SeitenHEMOPTISISJufrialdy AldyNoch keine Bewertungen
- Juvenile Nasopharyngeal Angiofibroma: Mehmet Fatih Garça, Sevil Ari Yuca, Köksal YucaDokument7 SeitenJuvenile Nasopharyngeal Angiofibroma: Mehmet Fatih Garça, Sevil Ari Yuca, Köksal YucaIkaKusumaWardhaniNoch keine Bewertungen
- Hemagioma SCDokument5 SeitenHemagioma SCCelebre MualabaNoch keine Bewertungen
- Jurnal Bedah SarafDokument10 SeitenJurnal Bedah SarafSarah AmaniNoch keine Bewertungen
- Conclusion: Long-Term Follow-Up ForDokument31 SeitenConclusion: Long-Term Follow-Up ForHima HuNoch keine Bewertungen
- Peripheral Nerve Blocks For Above Knee Amputation in High-Risk PatientsDokument7 SeitenPeripheral Nerve Blocks For Above Knee Amputation in High-Risk PatientstiobuanaNoch keine Bewertungen
- DSADokument7 SeitenDSANantini GopalNoch keine Bewertungen
- Percutaneous Aortic Valve Implantation: The Anesthesiologist PerspectiveDokument11 SeitenPercutaneous Aortic Valve Implantation: The Anesthesiologist Perspectiveserena7205Noch keine Bewertungen
- Pericardiectomy For Tuberculous Effusive-Constrictive PericarditisDokument5 SeitenPericardiectomy For Tuberculous Effusive-Constrictive PericarditisIJAR JOURNALNoch keine Bewertungen
- Bilateral External Carotid Artery Ligation A LifeDokument3 SeitenBilateral External Carotid Artery Ligation A LifeYoshua Eric IrawanNoch keine Bewertungen
- CE (Ra1) F (RK) PF1 (AJ SL RK) PN (P)Dokument4 SeitenCE (Ra1) F (RK) PF1 (AJ SL RK) PN (P)karthik padmanathanNoch keine Bewertungen
- An Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportDokument4 SeitenAn Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Application of Intracranial Pressure-Directed Therapy On DCIDokument9 SeitenApplication of Intracranial Pressure-Directed Therapy On DCIRonaldo MofuNoch keine Bewertungen
- Artigo HGF Neorologia Maio 2021Dokument11 SeitenArtigo HGF Neorologia Maio 2021Daniela MarinhoNoch keine Bewertungen
- Juvenile Nasopharyngeal AngiofibromaDokument16 SeitenJuvenile Nasopharyngeal AngiofibromaIren UbroNoch keine Bewertungen
- TTDokument11 SeitenTTRony palwagunaNoch keine Bewertungen
- Trauma EsplenicoDokument9 SeitenTrauma EsplenicoFelipe MayorcaNoch keine Bewertungen
- Extracorporeal Cardiopulmonary Resuscitation With Therapeutic Hypothermia For Prolonged Refractory In-Hospital Cardiac ArrestDokument10 SeitenExtracorporeal Cardiopulmonary Resuscitation With Therapeutic Hypothermia For Prolonged Refractory In-Hospital Cardiac Arrestika nur annisaNoch keine Bewertungen
- Jurnal SatyaDokument5 SeitenJurnal SatyaSatya WangsaNoch keine Bewertungen
- BCS NGT, Aspirasi AsitesDokument10 SeitenBCS NGT, Aspirasi AsitesSatya WangsaNoch keine Bewertungen
- Kasus:: Dka: Keton 5 Meq/L, Blood Glucose 250, PH 7.3, Ketonemia and Ketonuria, Serum Bicarbonate 18 Meq/L or LessDokument3 SeitenKasus:: Dka: Keton 5 Meq/L, Blood Glucose 250, PH 7.3, Ketonemia and Ketonuria, Serum Bicarbonate 18 Meq/L or LessSatya WangsaNoch keine Bewertungen
- 5 - ThrombopoiesisDokument3 Seiten5 - ThrombopoiesisSatya WangsaNoch keine Bewertungen
- Targeted Therapy in CancerDokument51 SeitenTargeted Therapy in CancerSatya WangsaNoch keine Bewertungen
- Wabah TBC Di IndiaDokument7 SeitenWabah TBC Di IndiaSatya WangsaNoch keine Bewertungen
- Wabah TBC Di VietnamDokument8 SeitenWabah TBC Di VietnamSatya WangsaNoch keine Bewertungen
- Biology Notes HSCDokument116 SeitenBiology Notes HSCYuki SuzukiNoch keine Bewertungen
- Micro HSB A - Myeloid Tissue HistologyDokument2 SeitenMicro HSB A - Myeloid Tissue HistologyGaelle Lisette MacatangayNoch keine Bewertungen
- GR 7 Ventures PEDokument232 SeitenGR 7 Ventures PEFaithNoch keine Bewertungen
- Types of Anaemia and How To Remember Them: With Sophie BroughtonDokument28 SeitenTypes of Anaemia and How To Remember Them: With Sophie BroughtonurtikikeNoch keine Bewertungen
- Pleading The Blood Is A Legal Thing!Dokument4 SeitenPleading The Blood Is A Legal Thing!Victor Ramlall100% (1)
- Group 7 Case StudyDokument4 SeitenGroup 7 Case StudyROSE GARETH SEGYEPNoch keine Bewertungen
- MANUAL ElectrophoresisDokument24 SeitenMANUAL ElectrophoresisMohamed Ali50% (2)
- Listening Script FullDokument93 SeitenListening Script FullkbalvinNoch keine Bewertungen
- Biopure Corporation - Pricing of OxyglobinDokument42 SeitenBiopure Corporation - Pricing of OxyglobinKotwal Mohit KotwalNoch keine Bewertungen
- MCQs On Respiration Physiology With KeyDokument7 SeitenMCQs On Respiration Physiology With KeyMudassar Roomi94% (31)
- 52 1023122 0 1Dokument7 Seiten52 1023122 0 1Kula Segara PandiyanNoch keine Bewertungen
- Sir Joseph Barcroft Obituario DHBarron Science1947Dokument2 SeitenSir Joseph Barcroft Obituario DHBarron Science1947Andrés MorenoNoch keine Bewertungen
- Warfarin Mechanism of Action, Indications AtfDokument4 SeitenWarfarin Mechanism of Action, Indications AtfAmir mohammad moori MohammadiNoch keine Bewertungen
- ( ) : Registration No.: Name (In English) : Class: Institution: Date of BirthDokument3 Seiten( ) : Registration No.: Name (In English) : Class: Institution: Date of Birtheverly.Noch keine Bewertungen
- Hematology NotesDokument3 SeitenHematology NotesFarisa Jane BanggoNoch keine Bewertungen
- Test Bank For Clinical Hematology and Fundamentals of Hemostasis 5th Edition HarmeningDokument6 SeitenTest Bank For Clinical Hematology and Fundamentals of Hemostasis 5th Edition HarmeningWilbur Penny100% (29)
- Book 9 PDFDokument33 SeitenBook 9 PDFMayuk KNoch keine Bewertungen
- Hematology Review NotesDokument28 SeitenHematology Review NoteszachNoch keine Bewertungen
- Minerals ChartDokument2 SeitenMinerals Chartautumn15_7Noch keine Bewertungen
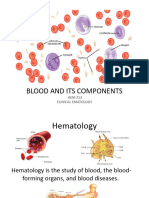
- Hematology Lecture 1 - Blood and Its Components - BackupDokument51 SeitenHematology Lecture 1 - Blood and Its Components - BackupHaizickNoch keine Bewertungen
- Clinical Guideline: Sepsis in PregnancyDokument24 SeitenClinical Guideline: Sepsis in PregnancyYerni DaeliNoch keine Bewertungen
- Lecture & Review Guide in HEMATOLOGY 1 & 2 (COMPLETE)Dokument58 SeitenLecture & Review Guide in HEMATOLOGY 1 & 2 (COMPLETE)Kirt Anonuevo100% (3)
- Pathology - Chapter 14Dokument14 SeitenPathology - Chapter 14Cory GrayNoch keine Bewertungen
- Dr. Norhafiza Saad-24 PagesDokument37 SeitenDr. Norhafiza Saad-24 PagesCallumNoch keine Bewertungen
- DLL - SCIENCE - Q2 - W2Dokument8 SeitenDLL - SCIENCE - Q2 - W2Carole FuentesNoch keine Bewertungen
- Concept MapDokument4 SeitenConcept MapDud AccNoch keine Bewertungen
- Lesson 4 Hydrostatic Pressure Osunero, Kim John S. BSED 2D SCIE 4Dokument4 SeitenLesson 4 Hydrostatic Pressure Osunero, Kim John S. BSED 2D SCIE 4Kim John OsuneroNoch keine Bewertungen
- IB Biology Option D - Human Physiology HL A3 Revision SheetDokument1 SeiteIB Biology Option D - Human Physiology HL A3 Revision SheetMarwan PharaonNoch keine Bewertungen
- Adequacy of Perfusion During Cardiopulmonary BypassDokument64 SeitenAdequacy of Perfusion During Cardiopulmonary BypassBranka Kurtovic50% (2)
- DK-The British Medical Association-Complete Family Health GuideDokument992 SeitenDK-The British Medical Association-Complete Family Health Guidedangnghia211290% (10)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedBewertung: 4 von 5 Sternen4/5 (61)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)