Das könnte Ihnen auch gefallen
- Trach care improves vital signs by removing secretionsDokument1 SeiteTrach care improves vital signs by removing secretionsdoirge47100% (8)
- Chart Smart - The a-To-Z Guide 3rdDokument507 SeitenChart Smart - The a-To-Z Guide 3rdDanae Jones100% (2)
- Examples - Registered Nurse Combined Self and Senior Nurse Assessment PDFDokument12 SeitenExamples - Registered Nurse Combined Self and Senior Nurse Assessment PDFamandeep kaur100% (2)
- Anatomy of a Super Nurse: The Ultimate Guide to Becoming NurseyVon EverandAnatomy of a Super Nurse: The Ultimate Guide to Becoming NurseyBewertung: 5 von 5 Sternen5/5 (3)
- Calculating Drug Dosages A Patient Safe Approach To Nursing and MathDokument564 SeitenCalculating Drug Dosages A Patient Safe Approach To Nursing and Mathkate96% (23)
- NCLEX Test Taking StrategiesDokument9 SeitenNCLEX Test Taking StrategiesLauren100% (4)
- Head Eyes: Head To Toe AssessmentDokument2 SeitenHead Eyes: Head To Toe AssessmentVijungco88% (8)
- Business Plan For LaboratoryDokument22 SeitenBusiness Plan For LaboratoryManish Rastogi100% (3)
- 150 Tips and Tricks for New Nurses: Balance a hectic schedule and get the sleep you need…Avoid illness and stay positive…Continue your education and keep up with medical advancesVon Everand150 Tips and Tricks for New Nurses: Balance a hectic schedule and get the sleep you need…Avoid illness and stay positive…Continue your education and keep up with medical advancesBewertung: 3 von 5 Sternen3/5 (6)
- Nclex Cheat SheetDokument9 SeitenNclex Cheat Sheetsophia onuNoch keine Bewertungen
- Physical Assessment Charting For NursingDokument7 SeitenPhysical Assessment Charting For NursingChristine Schroeder92% (13)
- Math For Nurses (Dosage Calculation)Dokument25 SeitenMath For Nurses (Dosage Calculation)Dennis B. Yap100% (7)
- Lean Process Improvement at Cleveland ClinicDokument20 SeitenLean Process Improvement at Cleveland ClinicSamNoch keine Bewertungen
- 17 Tips To Improve Your Nursing DocumentationDokument26 Seiten17 Tips To Improve Your Nursing DocumentationAgustin Lutfiana100% (1)
- Easy Nursing Notes For The Registered Nurse.Von EverandEasy Nursing Notes For The Registered Nurse.Bewertung: 4 von 5 Sternen4/5 (6)
- Key Nursing SkillsDokument359 SeitenKey Nursing Skillsmordanga100% (6)
- Nursing DocumentationDokument35 SeitenNursing DocumentationOktavia Milna Herlina100% (4)
- Nursing Skills Procedure ManualDokument154 SeitenNursing Skills Procedure ManualTina Talmadge100% (1)
- Communication Skills for Nurses: A Practical Guide on How to Achieve Successful ConsultationsVon EverandCommunication Skills for Nurses: A Practical Guide on How to Achieve Successful ConsultationsBewertung: 3.5 von 5 Sternen3.5/5 (6)
- PDFDokument416 SeitenPDFFerid Dauti100% (1)
- Nursing School Necessities Cheat SheetDokument3 SeitenNursing School Necessities Cheat SheetRevNoch keine Bewertungen
- Nursing Notes Templates (Guidelines To Take Nursing Notes)Dokument20 SeitenNursing Notes Templates (Guidelines To Take Nursing Notes)Rose100% (1)
- Nursing Assessment Cheat SheetDokument7 SeitenNursing Assessment Cheat Sheetanne009100% (2)
- PT 2 Nurse NotesDokument1 SeitePT 2 Nurse NotesAmy67% (3)
- Health AssessmentttDokument64 SeitenHealth AssessmentttAudreySalvador100% (4)
- The Nursing Assessment Cheat Sheet (ADPIE)Dokument3 SeitenThe Nursing Assessment Cheat Sheet (ADPIE)ajaz100% (1)
- NANDA Group ListDokument5 SeitenNANDA Group ListWahyu KristiyawanNoch keine Bewertungen
- Nursing Writing PDFDokument42 SeitenNursing Writing PDFRyu Tse50% (2)
- Nursing AssessmentDokument138 SeitenNursing AssessmentGhan Maria100% (1)
- Nurse Report Sheet SBARDokument4 SeitenNurse Report Sheet SBARBryan Nguyen50% (2)
- Nursing documentation essentialsDokument30 SeitenNursing documentation essentialsNdy MokaitNoch keine Bewertungen
- Proper Nursing Documentation WillDokument4 SeitenProper Nursing Documentation Willbel_dawn019Noch keine Bewertungen
- LPN NotesDokument223 SeitenLPN Notesandron1979100% (3)
- Care Planning & Reflection PresentationDokument48 SeitenCare Planning & Reflection PresentationBatool Al-ShabrakhaNoch keine Bewertungen
- Pku 3 Concept MapDokument3 SeitenPku 3 Concept Mapnursing concept maps100% (1)
- CHARTING BASICS GUIDEDokument11 SeitenCHARTING BASICS GUIDEfarahdlc100% (1)
- NursingDokument57 SeitenNursingremzylicious100% (1)
- Nursing Study Guide: Your Nursing Assistant To Do Well In SchoolVon EverandNursing Study Guide: Your Nursing Assistant To Do Well In SchoolBewertung: 3 von 5 Sternen3/5 (2)
- Nursing School Study ChecklistDokument8 SeitenNursing School Study Checklistmarisa joineNoch keine Bewertungen
- Picmonic NCLEX Study PlanDokument38 SeitenPicmonic NCLEX Study Planchellczy100% (1)
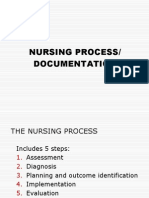
- Nursing Process and Documentation GuideDokument52 SeitenNursing Process and Documentation Guidegeorgeloto12100% (2)
- 2019 Nclex RN Cram SheetDokument20 Seiten2019 Nclex RN Cram Sheetrose angela100% (2)
- Nursing Documentation and Patient Record SystemDokument94 SeitenNursing Documentation and Patient Record SystemNomi Waqas GulNoch keine Bewertungen
- Boost critical thinking skills for NCLEX successDokument10 SeitenBoost critical thinking skills for NCLEX successTimbo Slice100% (1)
- Head To Toe Assessment Guide PDFDokument6 SeitenHead To Toe Assessment Guide PDFTashaNoch keine Bewertungen
- Steve M. Esteban RN, LPT, MSN, ManDokument39 SeitenSteve M. Esteban RN, LPT, MSN, ManSteve EstebanNoch keine Bewertungen
- Fundamentals of NursingDokument45 SeitenFundamentals of NursingCarrei Anne H. Duque100% (1)
- The Pearls For NCLEX Review PDFDokument32 SeitenThe Pearls For NCLEX Review PDFSandhu Sdhu100% (7)
- Dosage Calculations PacketDokument39 SeitenDosage Calculations PacketJack KeurigNoch keine Bewertungen
- How To Pass The NCLEX (FB Medical Alliedhealthbooks)Dokument15 SeitenHow To Pass The NCLEX (FB Medical Alliedhealthbooks)Aji Cruz-MataNoch keine Bewertungen
- The Everything New Nurse Book, 2nd Edition: Gain confidence, manage your schedule, and be ready for anything!Von EverandThe Everything New Nurse Book, 2nd Edition: Gain confidence, manage your schedule, and be ready for anything!Bewertung: 5 von 5 Sternen5/5 (1)
- Fundamentals1 Simple NursingDokument11 SeitenFundamentals1 Simple Nursingbetter be67% (3)
- Clinical Evaluation Process Nursing 3020Dokument9 SeitenClinical Evaluation Process Nursing 3020api-381845148Noch keine Bewertungen
- Nursing Study SitesDokument16 SeitenNursing Study Sitesspartacuslives100% (3)
- Navigating Nursing: A Practical Guide for the Novice Nurse from A to ZVon EverandNavigating Nursing: A Practical Guide for the Novice Nurse from A to ZNoch keine Bewertungen
- Complete Head-to-Toe Physical Assessment Cheat SheetDokument7 SeitenComplete Head-to-Toe Physical Assessment Cheat SheetA C100% (1)
- Basic Drug Cards 3Dokument14 SeitenBasic Drug Cards 3Karima Jones100% (1)
- Exam Facts NCLEX PN Nursing Study GuideVon EverandExam Facts NCLEX PN Nursing Study GuideBewertung: 3.5 von 5 Sternen3.5/5 (6)
- CRITICAL THINKING IN CLINICAL NURSING PRACTICE (RN): Passbooks Study GuideVon EverandCRITICAL THINKING IN CLINICAL NURSING PRACTICE (RN): Passbooks Study GuideNoch keine Bewertungen
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesVon EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesBewertung: 5 von 5 Sternen5/5 (1)
- PN FUNDAMENTALS: Passbooks Study GuideVon EverandPN FUNDAMENTALS: Passbooks Study GuideNoch keine Bewertungen
- Pave The Road To The Future of Application Development With Business ArchitectureDokument28 SeitenPave The Road To The Future of Application Development With Business ArchitectureTom KakanowskiNoch keine Bewertungen
- Communication and Collatboration Acute Care Mid-Point Reflective JournalDokument3 SeitenCommunication and Collatboration Acute Care Mid-Point Reflective Journalapi-346386230Noch keine Bewertungen
- RebeccaDokument2 SeitenRebeccaapi-422754271Noch keine Bewertungen
- Job Description: Chairman: Adrian Belton Chief Executive: Mrs Louise RobsonDokument11 SeitenJob Description: Chairman: Adrian Belton Chief Executive: Mrs Louise RobsonMohammad LouayNoch keine Bewertungen
- Nurs 604 Assignment 1 Critical Appraisal of An Advance Practice Role Final Copy For SubmissionDokument12 SeitenNurs 604 Assignment 1 Critical Appraisal of An Advance Practice Role Final Copy For Submissionapi-323169345Noch keine Bewertungen
- Resume - Afsaneh Sasani KoloriDokument2 SeitenResume - Afsaneh Sasani Kolorimohammadrezahajian12191Noch keine Bewertungen
- NMC Hospital Abu Dhabi - 2011!06!08Dokument16 SeitenNMC Hospital Abu Dhabi - 2011!06!08Manjul TakleNoch keine Bewertungen
- Great EasternDokument2 SeitenGreat EasternWeng Meng VISTANoch keine Bewertungen
- Industrial Practice On Networking For Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized HospitalDokument25 SeitenIndustrial Practice On Networking For Wachemo University Nigist Eleni Mohammed Memorial Comprehensive Specialized HospitalHasen Aumer100% (1)
- HNELHD CG 12 04 Warfarin Age Adjusted Dosing in AdultsDokument5 SeitenHNELHD CG 12 04 Warfarin Age Adjusted Dosing in AdultsAnonymous 4txA8N8etNoch keine Bewertungen
- PDF HealthDokument2 SeitenPDF HealthFarwa KhalidNoch keine Bewertungen
- Complementary Therapies in Clinical Practice: Helen BremnerDokument6 SeitenComplementary Therapies in Clinical Practice: Helen BremnersouthNoch keine Bewertungen
- TFN Faye AbdellahDokument48 SeitenTFN Faye AbdellahAbbeygale Galan100% (1)
- Ethical Issues in Service Quality PDFDokument16 SeitenEthical Issues in Service Quality PDFpiyushsithaNoch keine Bewertungen
- IHH Annual Report 2022Dokument144 SeitenIHH Annual Report 2022&Noch keine Bewertungen
- Elder CareDokument3 SeitenElder Caresushmma swarajaNoch keine Bewertungen
- Code of Medical Deontology of The Romanian College of PhysiciansDokument10 SeitenCode of Medical Deontology of The Romanian College of PhysiciansTeea EliadeNoch keine Bewertungen
- Checklist For Review of Floor Plan of Level 3 HospitalDokument7 SeitenChecklist For Review of Floor Plan of Level 3 HospitalOdessa Fortu LandichoNoch keine Bewertungen
- Functional NursingDokument2 SeitenFunctional NursingCharm TanyaNoch keine Bewertungen
- Quality Improvement Implementation SurveyDokument26 SeitenQuality Improvement Implementation SurveyShahRukh JhatialNoch keine Bewertungen
- Hospital Management System: A Mini Project Report OnDokument11 SeitenHospital Management System: A Mini Project Report OnPreethu GowdaNoch keine Bewertungen
- Bathe, Illness, Outpatient, Disability, Discharged, Geriatrics, Increase, Administer, Preventive, TherapyDokument3 SeitenBathe, Illness, Outpatient, Disability, Discharged, Geriatrics, Increase, Administer, Preventive, TherapyReka KutasiNoch keine Bewertungen
- Malabon Hospital Admission GuideDokument2 SeitenMalabon Hospital Admission GuideJose BernelNoch keine Bewertungen
- Nursing Reading 04Dokument2 SeitenNursing Reading 04Ge Lilian0% (1)
- Clinical Nursing Journal CapstoneDokument7 SeitenClinical Nursing Journal Capstoneapi-455776552Noch keine Bewertungen
- Your Medical Privacy ExplainedDokument6 SeitenYour Medical Privacy Explainedandrew tylerNoch keine Bewertungen
- Functions of OpdDokument3 SeitenFunctions of OpdAastha ShrivastavaNoch keine Bewertungen