Das könnte Ihnen auch gefallen
- Medical FormDokument4 SeitenMedical Formanisa aliNoch keine Bewertungen
- Employment Verification Form: The Department of Early Education and Care Subsidized Child CareDokument6 SeitenEmployment Verification Form: The Department of Early Education and Care Subsidized Child CareJessica PotratzNoch keine Bewertungen
- Health Systems Strengthening Participant Endorsement Form 2020Dokument1 SeiteHealth Systems Strengthening Participant Endorsement Form 2020Samuel WilliamsNoch keine Bewertungen
- Application Form MTCP PDFDokument8 SeitenApplication Form MTCP PDFrcalandriaNoch keine Bewertungen
- Cambridge Memorial Hospital Volunteer Association Application FormDokument6 SeitenCambridge Memorial Hospital Volunteer Association Application Formdaniela velascoNoch keine Bewertungen
- Allama Iqbal Open University: Aiou Student Support FundDokument2 SeitenAllama Iqbal Open University: Aiou Student Support FundMuhammad ShoaibNoch keine Bewertungen
- Nursing and Midwifery Registration Application.. UaeDokument4 SeitenNursing and Midwifery Registration Application.. UaeMadeleine Mae Garcia SalamatNoch keine Bewertungen
- Last First Middle InitialDokument3 SeitenLast First Middle InitialAsjsjsjsNoch keine Bewertungen
- COHP FamilyDokument4 SeitenCOHP FamilyAbigail Aracely Ochoa AlvaradoNoch keine Bewertungen
- Application Diploma Undergraduate 2015 2016Dokument5 SeitenApplication Diploma Undergraduate 2015 2016EM NemiNoch keine Bewertungen
- National Inurance Company Limited - Claim FormDokument3 SeitenNational Inurance Company Limited - Claim FormfuckyouprettyNoch keine Bewertungen
- Bipal Goyal - Release-Petition-FormDokument5 SeitenBipal Goyal - Release-Petition-FormBipal GoyalNoch keine Bewertungen
- Declaration of English Language Competencies 2B2Dokument1 SeiteDeclaration of English Language Competencies 2B2Ryan KadavilNoch keine Bewertungen
- NAIC Claim Form PDFDokument3 SeitenNAIC Claim Form PDFMohit BaggaNoch keine Bewertungen
- Sedgwick Logo - Certification of Health Care Provider For Family Member's Serious Health Condition (FMLA)Dokument4 SeitenSedgwick Logo - Certification of Health Care Provider For Family Member's Serious Health Condition (FMLA)teamirNoch keine Bewertungen
- 2021 HCSI ApplicationDokument10 Seiten2021 HCSI ApplicationmortensenkNoch keine Bewertungen
- HPV Consent - EnglishDokument1 SeiteHPV Consent - EnglishRosebery Andres ParroNoch keine Bewertungen
- Tower Sacco Education Scholarship Form 2024Dokument9 SeitenTower Sacco Education Scholarship Form 2024FOOTHILL CYBERNoch keine Bewertungen
- Crewsure Claim Form (XLCatlin) 1.3Dokument2 SeitenCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- Connecticut Nurse Midwife Pharmacology Course Verification FormDokument1 SeiteConnecticut Nurse Midwife Pharmacology Course Verification Formklwiley1Noch keine Bewertungen
- New India Assurance Hospitalisation Claim FormDokument3 SeitenNew India Assurance Hospitalisation Claim Formharshmanu1612Noch keine Bewertungen
- THC Information Sign-Up Form English Fillable ToolkitDokument2 SeitenTHC Information Sign-Up Form English Fillable ToolkitAsmaa El-emairyNoch keine Bewertungen
- Cps Deferment FormDokument1 SeiteCps Deferment Form1tonsilsNoch keine Bewertungen
- UERM ApplicationDokument5 SeitenUERM ApplicationJasper Benjamin JuradoNoch keine Bewertungen
- KSU Immunization Form 2016Dokument1 SeiteKSU Immunization Form 2016AminNoch keine Bewertungen
- CFPA-Medical ExpensesDokument2 SeitenCFPA-Medical ExpensesDivya VoletiNoch keine Bewertungen
- Application For Services PDFDokument9 SeitenApplication For Services PDFKyle LangsleyNoch keine Bewertungen
- 30 Medicl Procdur For ClaimDokument7 Seiten30 Medicl Procdur For Claimبلال خالدNoch keine Bewertungen
- EDSP Application FormDokument4 SeitenEDSP Application FormDave MillaresNoch keine Bewertungen
- Adventist College of Nursing & Health Sciences, Penang: For Office Use OnlyDokument3 SeitenAdventist College of Nursing & Health Sciences, Penang: For Office Use OnlyCarthieca tiecacueNoch keine Bewertungen
- International Observership Program Guidelines-Application-Credit Card-Immunization Record 2014Dokument15 SeitenInternational Observership Program Guidelines-Application-Credit Card-Immunization Record 2014drhassam90Noch keine Bewertungen
- Department of Education AND Department of Health Region IiiDokument1 SeiteDepartment of Education AND Department of Health Region IiiRej NicdaoNoch keine Bewertungen
- Scholarship Application Updated 120813Dokument4 SeitenScholarship Application Updated 120813api-221470498Noch keine Bewertungen
- Annexure-I Nomination/Registration Form - Applicants of Indian NationalityDokument8 SeitenAnnexure-I Nomination/Registration Form - Applicants of Indian NationalityRohitNoch keine Bewertungen
- G B A S A P 1 4: IVE ACK Mile Pplication AGE OFDokument4 SeitenG B A S A P 1 4: IVE ACK Mile Pplication AGE OFcancermoonwolfNoch keine Bewertungen
- KPC Inuka Scholarship Application Form 2024Dokument7 SeitenKPC Inuka Scholarship Application Form 202420goldfinch301Noch keine Bewertungen
- Jawad Claim FormDokument2 SeitenJawad Claim FormJawad KarimNoch keine Bewertungen
- CCTP Enrolment Form 7th 9th April 2014Dokument3 SeitenCCTP Enrolment Form 7th 9th April 2014GosfordCityRebelsNoch keine Bewertungen
- Pde 294Dokument6 SeitenPde 294marcusscoobyNoch keine Bewertungen
- Doctor Statement Ssa 787Dokument3 SeitenDoctor Statement Ssa 787Richard GuthNoch keine Bewertungen
- OJT-Application-formDokument3 SeitenOJT-Application-formSayong , John Mike J.Noch keine Bewertungen
- AIOU Student Support Fund DetailsDokument3 SeitenAIOU Student Support Fund Detailsfukanmaliq0% (1)
- Application 2011Dokument2 SeitenApplication 2011laltea2677Noch keine Bewertungen
- Section A: What Type of Coverage Are You Looking For?Dokument4 SeitenSection A: What Type of Coverage Are You Looking For?dewaankurNoch keine Bewertungen
- Rwo2 Application Form Edsp and Odsp For CollegeDokument4 SeitenRwo2 Application Form Edsp and Odsp For CollegeKarl Christian SupnetNoch keine Bewertungen
- Cooperative Health Enrollment FormDokument2 SeitenCooperative Health Enrollment FormGeraldine Daquipil TortalNoch keine Bewertungen
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDokument5 SeitenMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormrhvenkatNoch keine Bewertungen
- Exemption From Immunizations Form 3-23-23Dokument2 SeitenExemption From Immunizations Form 3-23-23Safeer UllahNoch keine Bewertungen
- Mass IMMUNIZATION RECORD Request FormDokument3 SeitenMass IMMUNIZATION RECORD Request Formwarriorsinrecoveryalex.rNoch keine Bewertungen
- Application Checklist and InstructionsDokument7 SeitenApplication Checklist and InstructionsISLAND NATANYANoch keine Bewertungen
- Self Cert FormDokument2 SeitenSelf Cert Formkevin kuhnNoch keine Bewertungen
- Adjunct Health Insurance Certification FormDokument2 SeitenAdjunct Health Insurance Certification FormElena GerashchenkoNoch keine Bewertungen
- Chiropractic Application Form: Section A: Contact InformationDokument6 SeitenChiropractic Application Form: Section A: Contact InformationAmanakeNoch keine Bewertungen
- CAP DiscApplicationFormENGDokument1 SeiteCAP DiscApplicationFormENGCee SNoch keine Bewertungen
- Dube Trade Port Application FormDokument7 SeitenDube Trade Port Application FormNcediswaNoch keine Bewertungen
- MedicalVerification PDFDokument3 SeitenMedicalVerification PDFOptical RecoveryNoch keine Bewertungen
- Request Summer AidDokument1 SeiteRequest Summer AidShauna LoveNoch keine Bewertungen
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsVon EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNoch keine Bewertungen
- How to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanVon EverandHow to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanNoch keine Bewertungen
- Research Coordinator ApplicationDokument1 SeiteResearch Coordinator Application2013alexizoNoch keine Bewertungen
- Job Description Ministry of Health Post: Health Education Officer (District Health Education Officer) Grade: Po/Cto QualificationsDokument1 SeiteJob Description Ministry of Health Post: Health Education Officer (District Health Education Officer) Grade: Po/Cto Qualifications2013alexizoNoch keine Bewertungen
- Pe Nams March3rDokument58 SeitenPe Nams March3r2013alexizoNoch keine Bewertungen
- Alex Chakhota Application EhoDokument1 SeiteAlex Chakhota Application Eho2013alexizoNoch keine Bewertungen
- PN April 2020Dokument14 SeitenPN April 20202013alexizoNoch keine Bewertungen
- Application Project ManagerDokument1 SeiteApplication Project Manager2013alexizoNoch keine Bewertungen
- Alex Chakhota Application Program OfficerDokument1 SeiteAlex Chakhota Application Program Officer2013alexizoNoch keine Bewertungen
- Alex Chakhota Monitoring and Evalution Spealist)Dokument1 SeiteAlex Chakhota Monitoring and Evalution Spealist)2013alexizoNoch keine Bewertungen
- Warning! Don't Nog GH Not Delete This Folder It Contains Folder Lock Encrypted DataDokument1 SeiteWarning! Don't Nog GH Not Delete This Folder It Contains Folder Lock Encrypted Data2013alexizoNoch keine Bewertungen
- Transport Ad orDokument1 SeiteTransport Ad orFredy20Noch keine Bewertungen
- Human Computer InteractionDokument12 SeitenHuman Computer Interactionabhi37Noch keine Bewertungen
- Production of Activated CarbonDokument11 SeitenProduction of Activated CarbonShii Bautista100% (1)
- Gil Sanchez, Labason Zamboanga Del Norte: AmacaDokument2 SeitenGil Sanchez, Labason Zamboanga Del Norte: AmacaMacky BirdNoch keine Bewertungen
- Washington State Employee - 4/2010Dokument8 SeitenWashington State Employee - 4/2010WFSEc28Noch keine Bewertungen
- G C Reddy ProfileDokument3 SeitenG C Reddy ProfileG.C.ReddyNoch keine Bewertungen
- 6 Hagonoy V NLRCDokument2 Seiten6 Hagonoy V NLRCChristiane Marie Bajada0% (1)
- ION8650 DatasheetDokument11 SeitenION8650 DatasheetAlthaf Axel HiroshiNoch keine Bewertungen
- E HANAAW 12 Sample QuestionDokument16 SeitenE HANAAW 12 Sample QuestionsuryaNoch keine Bewertungen
- Permit Part-2 Process-Oriented Permit in SAPDokument13 SeitenPermit Part-2 Process-Oriented Permit in SAPsachinWebDNoch keine Bewertungen
- Pg-586-591 - Annexure 13.1 - AllEmployeesDokument7 SeitenPg-586-591 - Annexure 13.1 - AllEmployeesaxomprintNoch keine Bewertungen
- Training and Development Project Report - MessDokument37 SeitenTraining and Development Project Report - MessIqra Bismi100% (1)
- Draft ASCE-AWEA RecommendedPracticeDokument72 SeitenDraft ASCE-AWEA RecommendedPracticeTeeBoneNoch keine Bewertungen
- Hutchinson - Le Joint Francais - National O-RingDokument25 SeitenHutchinson - Le Joint Francais - National O-RingkikorrasNoch keine Bewertungen
- 01 - Accounting For Managers PDFDokument151 Seiten01 - Accounting For Managers PDFAmit Kumar PandeyNoch keine Bewertungen
- The Importance of Personal Protective Equipment in Pesticide App 2018Dokument4 SeitenThe Importance of Personal Protective Equipment in Pesticide App 2018Anees MalikNoch keine Bewertungen
- Lecture 2 Leader-Centred PerspectivesDokument24 SeitenLecture 2 Leader-Centred PerspectivesLIVINGSTONE CAESARNoch keine Bewertungen
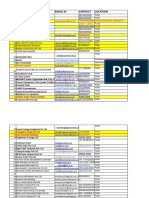
- Company Name Email Id Contact Location: 3 Praj Industries Limited Yogesh960488815Pune-Nagar Road, SanaswadiDokument65 SeitenCompany Name Email Id Contact Location: 3 Praj Industries Limited Yogesh960488815Pune-Nagar Road, SanaswadiDhruv Parekh100% (1)
- Wireshark Lab: 802.11: Approach, 6 Ed., J.F. Kurose and K.W. RossDokument5 SeitenWireshark Lab: 802.11: Approach, 6 Ed., J.F. Kurose and K.W. RossN Azzati LabibahNoch keine Bewertungen
- Project Report "A Study of Value Added Tax" "Kirloskar Oil Engines Limited" (Kirloskar Valve Plant)Dokument4 SeitenProject Report "A Study of Value Added Tax" "Kirloskar Oil Engines Limited" (Kirloskar Valve Plant)Sohel BangiNoch keine Bewertungen
- Unit 4: A World of Ideas: Learning CompassDokument3 SeitenUnit 4: A World of Ideas: Learning CompassRica Mae Lepiten MendiolaNoch keine Bewertungen
- Paper 19 Revised PDFDokument520 SeitenPaper 19 Revised PDFAmey Mehta100% (1)
- Poka Yoke BDokument31 SeitenPoka Yoke BjaymuscatNoch keine Bewertungen
- Black Bruin Hydraulic Motors On-Demand Wheel Drives EN CDokument11 SeitenBlack Bruin Hydraulic Motors On-Demand Wheel Drives EN CDiego AlbarracinNoch keine Bewertungen
- Interpretation 1Dokument17 SeitenInterpretation 1ysunnyNoch keine Bewertungen
- z2OrgMgmt FinalSummativeTest LearnersDokument3 Seitenz2OrgMgmt FinalSummativeTest LearnersJade ivan parrochaNoch keine Bewertungen
- CE 462 Construction ManagementDokument100 SeitenCE 462 Construction Managementmonicycle companyNoch keine Bewertungen
- Patient Safety IngDokument6 SeitenPatient Safety IngUlfani DewiNoch keine Bewertungen
- Risk Assessments-These Are The Risk Assessments Which Are Applicable To Works Onsite. Risk Definition and MatrixDokument8 SeitenRisk Assessments-These Are The Risk Assessments Which Are Applicable To Works Onsite. Risk Definition and MatrixTimothy AziegbemiNoch keine Bewertungen
- Proposed Construction of New Kutulo Airstrip - RetenderDokument112 SeitenProposed Construction of New Kutulo Airstrip - RetenderKenyaAirportsNoch keine Bewertungen
- Opening Up The Prescriptive Authority PipelineDokument10 SeitenOpening Up The Prescriptive Authority PipelineJohn GavazziNoch keine Bewertungen