Das könnte Ihnen auch gefallen
- Nursing Process in Administering MedicationsDokument37 SeitenNursing Process in Administering MedicationsLady Mae RamosNoch keine Bewertungen
- Clinical Pharmacy: Safe, Effective Use of MedicinesDokument19 SeitenClinical Pharmacy: Safe, Effective Use of MedicinesAnisha PandeyNoch keine Bewertungen
- Affa Textbook 9781284402803 FULL InteractivDokument368 SeitenAffa Textbook 9781284402803 FULL InteractivPia Alesci100% (3)
- Essential Pharmacology For Inpatient CareVon EverandEssential Pharmacology For Inpatient CareBewertung: 4.5 von 5 Sternen4.5/5 (7)
- Concept of Clinical PharmacyDokument30 SeitenConcept of Clinical PharmacyKishori Kedia100% (4)
- Clinical Pharmacy I: Defining the Role and ResponsibilitiesDokument38 SeitenClinical Pharmacy I: Defining the Role and ResponsibilitiesJurusan Farmasi Poltekkes MedanNoch keine Bewertungen
- 9 H q1 l1.2 The Concept of Community HealthDokument16 Seiten9 H q1 l1.2 The Concept of Community HealthRegine Rellores BaliatNoch keine Bewertungen
- Clinical Pharmacy IntroductionDokument36 SeitenClinical Pharmacy IntroductionHadassah ReyesNoch keine Bewertungen
- Clinical Pharmacy ServicesDokument60 SeitenClinical Pharmacy ServicesDr-Jagadeesh MangamooriNoch keine Bewertungen
- Adsorption PresentationDokument23 SeitenAdsorption Presentationarun231187100% (1)
- Irritable Bowel SyndromeDokument22 SeitenIrritable Bowel SyndromeMarium NabeelNoch keine Bewertungen
- Manpower Planning FinalDokument108 SeitenManpower Planning FinalDevi PrasannaNoch keine Bewertungen
- Work-Life Balance - Facebook Com LinguaLIBDokument257 SeitenWork-Life Balance - Facebook Com LinguaLIBDiegoAngeles100% (1)
- Complementary and Alternative Medicine (CAM) Supplement Use in People with Diabetes: A Clinician's Guide: A Clinician's GuideVon EverandComplementary and Alternative Medicine (CAM) Supplement Use in People with Diabetes: A Clinician's Guide: A Clinician's GuideNoch keine Bewertungen
- Dispensing ProcessDokument39 SeitenDispensing ProcessLyca Salarda100% (3)
- Carbohydrates 131204014552 Phpapp02 PDFDokument27 SeitenCarbohydrates 131204014552 Phpapp02 PDFTweenie Dalumpines100% (4)
- The Slim Book of Health Pearls: The Prevention of Medical ErrorsVon EverandThe Slim Book of Health Pearls: The Prevention of Medical ErrorsNoch keine Bewertungen
- Clinical Pharmacy PHR 405: Chapter 1: General ConsiderationsDokument24 SeitenClinical Pharmacy PHR 405: Chapter 1: General ConsiderationsSamiul Alam Rajib100% (1)
- Hands Only CPRDokument14 SeitenHands Only CPRabhieghailNoch keine Bewertungen
- Levothyroxine (Synthroid)Dokument1 SeiteLevothyroxine (Synthroid)E50% (2)
- ChromatographyDokument31 SeitenChromatographyarun231187Noch keine Bewertungen
- Basic of Self-Care and Non-Prescription DrugsDokument34 SeitenBasic of Self-Care and Non-Prescription DrugsMing Yew TingNoch keine Bewertungen
- Role of PharmacistDokument9 SeitenRole of PharmacistAbid Ali Khan0% (1)
- AHCC: The Medical Breakthrough in Natural ImmunotherapyVon EverandAHCC: The Medical Breakthrough in Natural ImmunotherapyBewertung: 5 von 5 Sternen5/5 (1)
- Nursing Process in Administering MedicationsDokument8 SeitenNursing Process in Administering MedicationsLady Mae Ramos94% (17)
- Boli Digestive Functionale 2018Dokument90 SeitenBoli Digestive Functionale 2018Cabel TeodorNoch keine Bewertungen
- Patient CounselingDokument26 SeitenPatient CounselingMeena AliNoch keine Bewertungen
- Introduction To PharmacologyDokument31 SeitenIntroduction To PharmacologyKobby AmoahNoch keine Bewertungen
- Drug DispensingDokument33 SeitenDrug DispensingchinecheremnfNoch keine Bewertungen
- Topic 5Dokument65 SeitenTopic 5deema dmdNoch keine Bewertungen
- Pelatihan Patient Counseling - Dr. Fita Rahmawati, SPFRS, AptDokument55 SeitenPelatihan Patient Counseling - Dr. Fita Rahmawati, SPFRS, AptLhyNa AiNun SofiaNoch keine Bewertungen
- Essentials of PharmacologyDokument26 SeitenEssentials of PharmacologyCharlene DeleonNoch keine Bewertungen
- Hospital pharmacy opportunities in ScotlandDokument40 SeitenHospital pharmacy opportunities in ScotlandKostas KoutsodimosNoch keine Bewertungen
- Lec 3 HospitalDokument13 SeitenLec 3 HospitalAya Eid 7asanNoch keine Bewertungen
- Dr. G Praveen KumarDokument36 SeitenDr. G Praveen KumarMuhammad Riaz BhattiNoch keine Bewertungen
- Clinical Pharmacy Introduction and ScopeDokument22 SeitenClinical Pharmacy Introduction and ScopeSufyan MirzaNoch keine Bewertungen
- CLINICAL PHARMACY OPTIMIZES PATIENT CARE THROUGH MEDICATION EXPERTISEDokument34 SeitenCLINICAL PHARMACY OPTIMIZES PATIENT CARE THROUGH MEDICATION EXPERTISEJoram David BeltranNoch keine Bewertungen
- Medication Safety With Tlan QuestionsDokument32 SeitenMedication Safety With Tlan QuestionsKay KayNoch keine Bewertungen
- Desak Ernawati., PHD., Apt Pharmacology and Therapeutics DepartmentDokument47 SeitenDesak Ernawati., PHD., Apt Pharmacology and Therapeutics DepartmentyharobbiNoch keine Bewertungen
- Rational Drug Therapy GuideDokument36 SeitenRational Drug Therapy GuideVenu D DonNoch keine Bewertungen
- PharmD Orientation GuideDokument30 SeitenPharmD Orientation GuideDr-Md Abul Barkat100% (1)
- PW Principles and PracticesDokument56 SeitenPW Principles and PracticesBeena ShajimonNoch keine Bewertungen
- Pharmacy Orientation PPP211: Introduction To The Pharmacy Profession and The Future of The PharmacistDokument27 SeitenPharmacy Orientation PPP211: Introduction To The Pharmacy Profession and The Future of The PharmacistJape GarridoNoch keine Bewertungen
- Kie Dan KonselingDokument64 SeitenKie Dan KonselingPaten PisanNoch keine Bewertungen
- Internship ReportDokument43 SeitenInternship ReportCarissetotz Tan0% (1)
- Professional responsibilities of pharmacistsDokument5 SeitenProfessional responsibilities of pharmacistsShehnaz SheikhNoch keine Bewertungen
- Week 7 - PHR514-Pharmacy Law and Regulatory AffairsDokument31 SeitenWeek 7 - PHR514-Pharmacy Law and Regulatory AffairsNeymar ShuvoNoch keine Bewertungen
- Pharmaceutical Care ConceptDokument38 SeitenPharmaceutical Care ConceptTiti SulistiowatiNoch keine Bewertungen
- Pharmacy OrientationDokument23 SeitenPharmacy OrientationMohan AnwarNoch keine Bewertungen
- Pharmaceutical Care Process:: Assessment - Care Plan - Follow UpDokument54 SeitenPharmaceutical Care Process:: Assessment - Care Plan - Follow UpRaharjo AdityaNoch keine Bewertungen
- A Guide To Patient Medication Review: September 2003Dokument33 SeitenA Guide To Patient Medication Review: September 2003Muhamad GunturNoch keine Bewertungen
- Hospital Pharmacy PresentationDokument154 SeitenHospital Pharmacy PresentationKen OviedoNoch keine Bewertungen
- Medication Administration and Drug CalculationsDokument30 SeitenMedication Administration and Drug CalculationsPinkulal KaranNoch keine Bewertungen
- Prescription and abbreviationDokument54 SeitenPrescription and abbreviationsanjeev khanalNoch keine Bewertungen
- Good Prescribing Guide: Rational Treatment Process & Selecting Appropriate DrugsDokument20 SeitenGood Prescribing Guide: Rational Treatment Process & Selecting Appropriate Drugsbil sitNoch keine Bewertungen
- Prescription WrittingDokument26 SeitenPrescription WrittingJoseline AliceNoch keine Bewertungen
- Intern RoundsDokument24 SeitenIntern Roundsapi-381827675Noch keine Bewertungen
- Career Pharmacy AssignmentDokument9 SeitenCareer Pharmacy AssignmentLAIBA REHMANNoch keine Bewertungen
- Safety and Quality of Drug AdminstrationDokument5 SeitenSafety and Quality of Drug Adminstrationaddison.valerio09Noch keine Bewertungen
- Administering MedicationsDokument24 SeitenAdministering MedicationsCharmie GandaNoch keine Bewertungen
- Medication Administration GuideDokument204 SeitenMedication Administration GuidesaheedvkNoch keine Bewertungen
- Concrete ExamplesDokument84 SeitenConcrete ExamplesHERLIN HOBAYANNoch keine Bewertungen
- Career OptionsDokument28 SeitenCareer OptionsFaizan DonNoch keine Bewertungen
- Pharmacology For Nursing. Richard A. LehneDokument62 SeitenPharmacology For Nursing. Richard A. LehneJC Ortiz-Carrillo50% (2)
- 5 Role of Pharmacist in PHDokument20 Seiten5 Role of Pharmacist in PHمحمد العمريNoch keine Bewertungen
- ESA Medication-ErrorDokument22 SeitenESA Medication-ErrorMarius PapuricaNoch keine Bewertungen
- Ada Clin PharmDokument137 SeitenAda Clin Pharmkritikalgaming08Noch keine Bewertungen
- 1 Dr. Erwin Astha T - Bpjs Jatim 2016Dokument41 Seiten1 Dr. Erwin Astha T - Bpjs Jatim 2016Diah AzarineNoch keine Bewertungen
- M5 Continuation Dispensing ProcessDokument32 SeitenM5 Continuation Dispensing Processcbun22222Noch keine Bewertungen
- Pharma Lesson 1Dokument3 SeitenPharma Lesson 1BabyJane GRomeroNoch keine Bewertungen
- PhysiologicalrolesofmineralsDokument46 SeitenPhysiologicalrolesofmineralsarun231187Noch keine Bewertungen
- XRDDokument27 SeitenXRDHardik PrajapatiNoch keine Bewertungen
- Composition and FunctionsDokument13 SeitenComposition and Functionsarun231187Noch keine Bewertungen
- Paperchromatographybharmsud 151012115319 Lva1 App6891 PDFDokument34 SeitenPaperchromatographybharmsud 151012115319 Lva1 App6891 PDFarun231187Noch keine Bewertungen
- PUB210 HemeAtlas SampleDokument6 SeitenPUB210 HemeAtlas Samplearun231187Noch keine Bewertungen
- Conductometry Titrations PDFDokument4 SeitenConductometry Titrations PDFkomalseemi97Noch keine Bewertungen
- International University of Africa Faculty of Pharmacy Medicinal Chemistry MCHM 311 Siddieg Omer Elsiddieg, M. SC, B. SC (Honors)Dokument47 SeitenInternational University of Africa Faculty of Pharmacy Medicinal Chemistry MCHM 311 Siddieg Omer Elsiddieg, M. SC, B. SC (Honors)arun231187Noch keine Bewertungen
- Specific Immune System: T - LymphocytesDokument18 SeitenSpecific Immune System: T - Lymphocytesarun231187Noch keine Bewertungen
- Vogel ExtractDokument17 SeitenVogel Extractarun231187Noch keine Bewertungen
- Ureacycle ConversionDokument31 SeitenUreacycle Conversionarun231187Noch keine Bewertungen
- Calibracion MicropipetasDokument4 SeitenCalibracion MicropipetasAnonymous 58LGc3Noch keine Bewertungen
- TwocomponentsystemDokument28 SeitenTwocomponentsystemarun231187Noch keine Bewertungen
- Introduction to Biochemistry FundamentalsDokument34 SeitenIntroduction to Biochemistry Fundamentalsarun231187Noch keine Bewertungen
- ThephaseruleDokument48 SeitenThephaserulearun231187Noch keine Bewertungen
- 4 ImportanceofbiochemistryDokument18 Seiten4 Importanceofbiochemistryarun231187Noch keine Bewertungen
- High Energy Compouds: Anjali.H.S BCH.10.05.10Dokument66 SeitenHigh Energy Compouds: Anjali.H.S BCH.10.05.10arun231187Noch keine Bewertungen
- StalagmometerDokument4 SeitenStalagmometerRamesh KumarNoch keine Bewertungen
- Pipette CalibrationDokument79 SeitenPipette Calibrationarun231187Noch keine Bewertungen
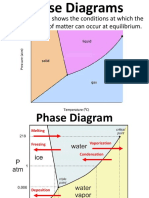
- A Phase Diagram Shows The Conditions at Which The Distinct Phases of Matter Can Occur at EquilibriumDokument9 SeitenA Phase Diagram Shows The Conditions at Which The Distinct Phases of Matter Can Occur at Equilibriumarun231187Noch keine Bewertungen
- CARBOHYDRATESDokument38 SeitenCARBOHYDRATESgulrukh100% (3)
- Titrasi PresipitasiDokument85 SeitenTitrasi PresipitasiayukiwaNoch keine Bewertungen
- Carpalbonefractures 150330093618 Conversion Gate01Dokument136 SeitenCarpalbonefractures 150330093618 Conversion Gate01arun231187Noch keine Bewertungen
- Pipette CalibrationDokument4 SeitenPipette CalibrationbalajivangaruNoch keine Bewertungen
- Nutrition 1101-Lecture 21Dokument21 SeitenNutrition 1101-Lecture 21arun231187Noch keine Bewertungen
- Qualitative Carbohydrate Tests GuideDokument52 SeitenQualitative Carbohydrate Tests Guidearun231187Noch keine Bewertungen
- 4 ImportanceofbiochemistryDokument18 Seiten4 Importanceofbiochemistryarun231187Noch keine Bewertungen
- Tsca Toxic Substanteces Control ActDokument1 SeiteTsca Toxic Substanteces Control ActAlbert Casanova FernandezNoch keine Bewertungen
- Bilingual RNs Reduce Costs, Improve Satisfaction and Readmission Rates, Reduce ER Wait TimesDokument1 SeiteBilingual RNs Reduce Costs, Improve Satisfaction and Readmission Rates, Reduce ER Wait TimesInstitute of CaliforniaNoch keine Bewertungen
- HypotrophyDokument3 SeitenHypotrophyopeyemi daramolaNoch keine Bewertungen
- WB CE Act Registration RegulationDokument42 SeitenWB CE Act Registration RegulationDipak Ranjan MukherjeeNoch keine Bewertungen
- Epididymo OrchitisDokument20 SeitenEpididymo OrchitisDurai Raj Kumar100% (2)
- 3 Public Health ApproachDokument61 Seiten3 Public Health Approachdawit tesfaNoch keine Bewertungen
- 10 WinterDokument48 Seiten10 WintercontinentdriftNoch keine Bewertungen
- Chemical Handling and ManagementDokument22 SeitenChemical Handling and Managementrizwan chNoch keine Bewertungen
- Exercise CH 04Dokument9 SeitenExercise CH 04Nurshuhada Nordin0% (1)
- خارطة اختبار الترميز الطبيDokument3 Seitenخارطة اختبار الترميز الطبيANFALNoch keine Bewertungen
- Ebola Virus HOMEOPHATYDokument3 SeitenEbola Virus HOMEOPHATYgiopscribdNoch keine Bewertungen
- Perioperative Nursing 101Dokument2 SeitenPerioperative Nursing 101Anthony Dema-ala0% (1)
- Main Match Results and Data 2014Dokument116 SeitenMain Match Results and Data 2014joe_egypt_866088307100% (1)
- Uganda Universities and Courses For Student Loan SupportDokument5 SeitenUganda Universities and Courses For Student Loan SupportThe Campus TimesNoch keine Bewertungen
- Leadership Accountability Nurs631Dokument6 SeitenLeadership Accountability Nurs631api-241398334Noch keine Bewertungen
- Valid and Ethical Use of Psych AssessmentDokument2 SeitenValid and Ethical Use of Psych AssessmentEJNoch keine Bewertungen
- WHO MBHSS 2010 Section2 Web PDFDokument20 SeitenWHO MBHSS 2010 Section2 Web PDFDnrxsNoch keine Bewertungen
- 2014 Windsor University Commencement Ceremony PROOFDokument28 Seiten2014 Windsor University Commencement Ceremony PROOFKeidren LewiNoch keine Bewertungen
- 三民高三上第二次月考複習 教師卷Dokument12 Seiten三民高三上第二次月考複習 教師卷黃紘志Noch keine Bewertungen
- Spider AngiomaDokument5 SeitenSpider AngiomaVishal SharmaNoch keine Bewertungen
- Improving Performance and Outcomes: Section 7Dokument4 SeitenImproving Performance and Outcomes: Section 7Andrew WongNoch keine Bewertungen
- Alprazolam PoisoningDokument4 SeitenAlprazolam PoisoningRahmat AkmalNoch keine Bewertungen