Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Kurt Cobain Case StudyDokument11 SeitenKurt Cobain Case StudyKC Respicio67% (3)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- CPC Exam Review QuestionsDokument3 SeitenCPC Exam Review QuestionshevinpatelNoch keine Bewertungen
- Fish & Shellfish PoisoningDokument29 SeitenFish & Shellfish Poisoningkolita kamal100% (4)
- The Digestive System and its ProcessesDokument5 SeitenThe Digestive System and its ProcessesRavenApigoNoch keine Bewertungen
- Litrature & Case StudyDokument74 SeitenLitrature & Case Studynaol buloNoch keine Bewertungen
- Typhoid Fever NCPDokument46 SeitenTyphoid Fever NCPLyra Lustre RN67% (3)
- Neonatal Emergencies FinalDokument90 SeitenNeonatal Emergencies FinalDr Raseena VattamkandathilNoch keine Bewertungen
- Case Study PneumothoraxDokument9 SeitenCase Study PneumothoraxLee_Cabral_693967% (3)
- Smart + Smart Enhancer: Medic MedicDokument11 SeitenSmart + Smart Enhancer: Medic MedicmiazainuddinNoch keine Bewertungen
- Minimum Inhibitory ConcentrationDokument7 SeitenMinimum Inhibitory ConcentrationToshio HamazakiNoch keine Bewertungen
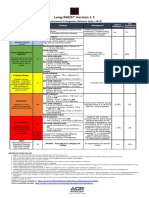
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokument1 SeiteLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNoch keine Bewertungen
- Windkessel EffectDokument11 SeitenWindkessel EffectAkhmad HidayatNoch keine Bewertungen
- Rheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009Dokument9 SeitenRheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009drwstokes100% (1)
- Acute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsDokument2 SeitenAcute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsSachin SinghNoch keine Bewertungen
- 020 - Metabolism of Proteins 3Dokument12 Seiten020 - Metabolism of Proteins 3Sargonan RaviNoch keine Bewertungen
- Complications of 3rd TrimesterDokument49 SeitenComplications of 3rd TrimesterMA. JYRELL BONITONoch keine Bewertungen
- Critical Thinking Case Study #18:: Sickle-Cell AnemiaDokument15 SeitenCritical Thinking Case Study #18:: Sickle-Cell AnemiaHakima Hadji DaudNoch keine Bewertungen
- TimeWise Miracle Set 3D Fact Sheet MYSG ENGDokument2 SeitenTimeWise Miracle Set 3D Fact Sheet MYSG ENGKilinSilinNoch keine Bewertungen
- Bronchopulmonary Dysplasia (BPD)Dokument13 SeitenBronchopulmonary Dysplasia (BPD)Joan BuiNoch keine Bewertungen
- Remote Area Nursing Emergency GuidelinesDokument325 SeitenRemote Area Nursing Emergency Guidelineslavinia_dobrescu_1Noch keine Bewertungen
- Nursing Management - Colon CancerDokument7 SeitenNursing Management - Colon CancerReese Alessandra GandulfoNoch keine Bewertungen
- 13 - Adverse Drug Reactions CausesDokument4 Seiten13 - Adverse Drug Reactions CausesRojas Evert AlonsoNoch keine Bewertungen
- Case Report模板Dokument18 SeitenCase Report模板ChenNoch keine Bewertungen
- FormsDokument15 SeitenFormsBiswajit DasNoch keine Bewertungen
- COVID-19 Patient Report SummaryDokument2 SeitenCOVID-19 Patient Report Summarymuhammad imranNoch keine Bewertungen
- rút gọnDokument3 Seitenrút gọnUyen VuNoch keine Bewertungen
- Necrotizing Soft Tissue Infections GuideDokument21 SeitenNecrotizing Soft Tissue Infections GuideHen RyNoch keine Bewertungen
- Leaflet YTiG Plus Tablet For CHCDokument1 SeiteLeaflet YTiG Plus Tablet For CHCDesi Health Tips UpdateNoch keine Bewertungen
- 17-6 eJDD FinalDokument100 Seiten17-6 eJDD FinalMohamed GamalNoch keine Bewertungen
- List of Empanelled Hospitals in CGHS NagpurDokument58 SeitenList of Empanelled Hospitals in CGHS NagpurRajatNoch keine Bewertungen