Das könnte Ihnen auch gefallen
- Sommeil: Les Grands Articles d'UniversalisVon EverandSommeil: Les Grands Articles d'UniversalisNoch keine Bewertungen
- Supliment NEUROLOGIE PDFDokument32 SeitenSupliment NEUROLOGIE PDFnmona86Noch keine Bewertungen
- Neurological Assessment From Birth To 6Dokument22 SeitenNeurological Assessment From Birth To 6Ioana Panait-VasiliuNoch keine Bewertungen
- Pathologie Neurologique Périnatale Et Ses ConséquencesDokument272 SeitenPathologie Neurologique Périnatale Et Ses ConséquencesAnes ArcNoch keine Bewertungen
- 0710 Reanimation Vol16 N6 p546 - 552Dokument7 Seiten0710 Reanimation Vol16 N6 p546 - 552dragon man sportNoch keine Bewertungen
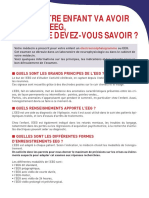
- Votre Enfant Va Avoir Un Eeg, Que Devez-Vous Savoir ?: Quels Sont Les Grands Principes de L'Eeg ?Dokument8 SeitenVotre Enfant Va Avoir Un Eeg, Que Devez-Vous Savoir ?: Quels Sont Les Grands Principes de L'Eeg ?Chaimae AouadNoch keine Bewertungen
- État de Vigilance Cycle Veille Sommeil PDFDokument58 SeitenÉtat de Vigilance Cycle Veille Sommeil PDFBMA-medecineNoch keine Bewertungen
- UE2 Tome 4 Sur 4Dokument145 SeitenUE2 Tome 4 Sur 4mathieu.lanier.2004Noch keine Bewertungen
- Veille SommeilDokument8 SeitenVeille Sommeilkhouloud djebabraNoch keine Bewertungen
- VEILLE ET SOMMEIL Par 2 DiaposDokument23 SeitenVEILLE ET SOMMEIL Par 2 DiaposRaphaël BikoahNoch keine Bewertungen
- Electroencéphalographie: I. DéfinitionDokument3 SeitenElectroencéphalographie: I. DéfinitionImane AkrchNoch keine Bewertungen
- Exploration Neurophysiologique Chez L - Enfant 2014Dokument23 SeitenExploration Neurophysiologique Chez L - Enfant 2014Yacine YacineNoch keine Bewertungen
- Eeg Etat de Mal GelisseDokument6 SeitenEeg Etat de Mal GelisseHAKIMOPNoch keine Bewertungen
- Ejsr 79 1 14Dokument16 SeitenEjsr 79 1 14hafidmedyaz7Noch keine Bewertungen
- L'épilepsie de L'enfant PDFDokument52 SeitenL'épilepsie de L'enfant PDFOmar FilozofNoch keine Bewertungen
- Le SommeilDokument10 SeitenLe SommeilMichael GuillienNoch keine Bewertungen
- Cours 1 IMC PHYSIO 2017Dokument18 SeitenCours 1 IMC PHYSIO 2017sawssenNoch keine Bewertungen
- Infirmite Motrice CerebraleDokument44 SeitenInfirmite Motrice CerebraleMaria Dumitrica100% (1)
- 7-Cycle Veille-SommeilDokument21 Seiten7-Cycle Veille-Sommeilyaya camaraNoch keine Bewertungen
- Dubois Revue Neurophyclin12Dokument10 SeitenDubois Revue Neurophyclin12Nounou NouhadeNoch keine Bewertungen
- FichesCerveau SommeilDokument4 SeitenFichesCerveau SommeilStéphane MaliyamunguNoch keine Bewertungen
- Traduction Classif Crises Epi Nouveau NeDokument19 SeitenTraduction Classif Crises Epi Nouveau Nebransiroudayna9Noch keine Bewertungen
- Cours de Psychophysiologie N°8Dokument13 SeitenCours de Psychophysiologie N°8Mezian BelkacemiNoch keine Bewertungen
- Exposé Benabdsellam (NSC)Dokument9 SeitenExposé Benabdsellam (NSC)Menaoum DalilaNoch keine Bewertungen
- Examen Échographique Du Système Nerveux Central Du Fœtus: Lignes Directrices Pour Effectuer L'examen de Dépistage Et Le Neurosonogramme FœtalDokument19 SeitenExamen Échographique Du Système Nerveux Central Du Fœtus: Lignes Directrices Pour Effectuer L'examen de Dépistage Et Le Neurosonogramme FœtalMartine MAILLOTNoch keine Bewertungen
- Chapitre 3 - IEF NeurologiqueDokument44 SeitenChapitre 3 - IEF Neurologiquezenazel miloudNoch keine Bewertungen
- L Electro EncephalogrammeDokument49 SeitenL Electro EncephalogrammeBehard KabeyaNoch keine Bewertungen
- Fichier Produit 2295Dokument10 SeitenFichier Produit 2295Caroline NganbouhNoch keine Bewertungen
- Fiches CODEX MAJ 05-05-2023Dokument124 SeitenFiches CODEX MAJ 05-05-2023pianodu21Noch keine Bewertungen
- BILAN PRECHIRURGICAL EPILEPSY (I.Bedoui) 2020 PDFDokument9 SeitenBILAN PRECHIRURGICAL EPILEPSY (I.Bedoui) 2020 PDFIchrak GhachemNoch keine Bewertungen
- Pratique de l'EEG PDFDokument217 SeitenPratique de l'EEG PDFOmar EL Fakir100% (3)
- La Rééducation Vestibulaire: Ana TomieDokument6 SeitenLa Rééducation Vestibulaire: Ana Tomiekarim.acpeNoch keine Bewertungen
- L'évolution À Long Terme Des Encéphalopathies ÉpileptiquesDokument10 SeitenL'évolution À Long Terme Des Encéphalopathies ÉpileptiquesRachid RazzoukiNoch keine Bewertungen
- Affections Mentales Chap6 PappDokument128 SeitenAffections Mentales Chap6 PappLorenaNoch keine Bewertungen
- TachesDokument44 SeitenTachesiangechancelleNoch keine Bewertungen
- Contrôle Postural Chez L'enfant Dyslexique Effet D'une Double TâcheDokument1 SeiteContrôle Postural Chez L'enfant Dyslexique Effet D'une Double TâcheRachid RazzoukiNoch keine Bewertungen
- D.legeR - Horloge BiologiqueDokument37 SeitenD.legeR - Horloge BiologiqueMihaela-Alexandra PopNoch keine Bewertungen
- Perceptions Illusoires de Son Propre Corps Par Stimulation CorticaleDokument3 SeitenPerceptions Illusoires de Son Propre Corps Par Stimulation CorticaleJean-Guy DuboisNoch keine Bewertungen
- Encephalopathie Hypoxo Ischemique Du Ne A Terme Diagnostic Orientation Et Prise en ChargeDokument13 SeitenEncephalopathie Hypoxo Ischemique Du Ne A Terme Diagnostic Orientation Et Prise en ChargeSublime MabeletNoch keine Bewertungen
- Physiologie Du Sommeil PDFDokument13 SeitenPhysiologie Du Sommeil PDFAbdelhak CheghibNoch keine Bewertungen
- VertigesDokument28 SeitenVertigesMylNoch keine Bewertungen
- Physiologie Du Cycle Veille - Sommeil ArameDokument43 SeitenPhysiologie Du Cycle Veille - Sommeil ArameSafae MaaroufNoch keine Bewertungen
- CC Expose PPDokument10 SeitenCC Expose PPHectarmaNoch keine Bewertungen
- Enfants Et LumièreDokument14 SeitenEnfants Et Lumièretitipim360Noch keine Bewertungen
- $ Degenerescence Pigmentaire de La Rétine $$Dokument7 Seiten$ Degenerescence Pigmentaire de La Rétine $$superser123465Noch keine Bewertungen
- Sommeil TheorieDokument90 SeitenSommeil TheorieMidorfiNoch keine Bewertungen
- Exemple Généralités EEGDokument17 SeitenExemple Généralités EEGIkram TenaniNoch keine Bewertungen
- EEGCNEDokument2 SeitenEEGCNEFtiho ChouNoch keine Bewertungen
- EEGCNEDokument2 SeitenEEGCNEFtiho ChouNoch keine Bewertungen
- Imagerie Des Surrénales de L'enfantDokument36 SeitenImagerie Des Surrénales de L'enfantabdouleNoch keine Bewertungen
- Epilepsie Et Sommeil Des Neurologie DR Stal 2017 PDFDokument40 SeitenEpilepsie Et Sommeil Des Neurologie DR Stal 2017 PDFShanito Not'onbut'offNoch keine Bewertungen
- Synthese BFEMDokument27 SeitenSynthese BFEMnianghadiaw248Noch keine Bewertungen
- Continuum Veille SommeilDokument66 SeitenContinuum Veille SommeilPanandba NikiemaNoch keine Bewertungen
- CHN William Lennox - Fiche Pratique - EegDokument1 SeiteCHN William Lennox - Fiche Pratique - EegBarkousNoch keine Bewertungen
- 10 Convulsions NNDokument44 Seiten10 Convulsions NNBenzaoui DjemanaNoch keine Bewertungen
- Sommeil Un Carnet Pour Mieux ComprendreDokument28 SeitenSommeil Un Carnet Pour Mieux Comprendrelepresse Damien100% (1)
- Systeme Nerveux CentralDokument19 SeitenSysteme Nerveux CentralBRAKNESSNoch keine Bewertungen
- Neurophysio de La FCT ProprioceptiveDokument8 SeitenNeurophysio de La FCT ProprioceptiveImane BenderazNoch keine Bewertungen
- Convulsions de L'enfantDokument22 SeitenConvulsions de L'enfantwooden latexNoch keine Bewertungen
- Perfetti 1Dokument9 SeitenPerfetti 1Kouloud GuibenNoch keine Bewertungen
- Apport Diagnostique Du Lavage Broncho-Alvéolaire Hilario NunesDokument65 SeitenApport Diagnostique Du Lavage Broncho-Alvéolaire Hilario NunesIna GrecuNoch keine Bewertungen
- De La Plaie Au Pansement-1Dokument5 SeitenDe La Plaie Au Pansement-1Jalal ManchorNoch keine Bewertungen
- Article4 37Dokument7 SeitenArticle4 37شهد 'ےNoch keine Bewertungen
- Lesiteducapaepe Pse Corrige-Metropole2021Dokument11 SeitenLesiteducapaepe Pse Corrige-Metropole2021yama1976saoNoch keine Bewertungen
- SI Fixateur ExterneDokument7 SeitenSI Fixateur ExterneAhmed FellagNoch keine Bewertungen
- Hypotensions OrhostatiquesDokument6 SeitenHypotensions OrhostatiquesDjallal HassaniNoch keine Bewertungen
- La RadiotherapieDokument10 SeitenLa RadiotherapieSouhayl ChouaaibNoch keine Bewertungen
- Organisation Technique - Ministère de La Santé PubliqueDokument4 SeitenOrganisation Technique - Ministère de La Santé PubliquemariemNoch keine Bewertungen
- Duratears Pommade Ophtalmique Pommade 3 5gDokument5 SeitenDuratears Pommade Ophtalmique Pommade 3 5gNobl InessNoch keine Bewertungen
- MemoireDokument108 SeitenMemoireZaki RamoulNoch keine Bewertungen
- Orthopédie Pédiatrique Et RéeducationDokument21 SeitenOrthopédie Pédiatrique Et RéeducationMay Znati33% (3)
- 1EnsSci 4047a Sujet Curietherapie 0Dokument3 Seiten1EnsSci 4047a Sujet Curietherapie 0DelcourtNoch keine Bewertungen
- Reflexology Health History WebsiteDokument2 SeitenReflexology Health History WebsitedinaNoch keine Bewertungen
- 2022-01-06 Note Methodo MutationDokument5 Seiten2022-01-06 Note Methodo MutationBaba DravignyNoch keine Bewertungen
- Habilitation BacteriologieDokument2 SeitenHabilitation BacteriologieToto FollyNoch keine Bewertungen
- Syndromes NéphrologiquesDokument40 SeitenSyndromes NéphrologiquesMahmoud KammounNoch keine Bewertungen
- RéflexologieDokument3 SeitenRéflexologieIna Ursu-Zatic0% (1)
- ETHIQUEDokument6 SeitenETHIQUEMENGA MENGA patrickNoch keine Bewertungen
- MTEV Chez Femme EnceinteDokument23 SeitenMTEV Chez Femme EnceinteSFA_ANGEIOLOGIE100% (1)
- UE 2.11 Les Traitements de Lappareil RespiratoireDokument18 SeitenUE 2.11 Les Traitements de Lappareil RespiratoireBruce DO VANNoch keine Bewertungen
- CMD CMG 3fev21Dokument21 SeitenCMD CMG 3fev21Aboubacar ToureNoch keine Bewertungen
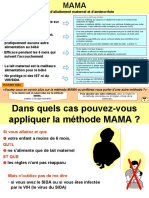
- 17 MamaDokument6 Seiten17 MamaJude EmmanuelNoch keine Bewertungen
- PRODUITS SQNGUINS UCcours N°2 PDFDokument21 SeitenPRODUITS SQNGUINS UCcours N°2 PDFsoumri omaimaNoch keine Bewertungen
- 27 Les CardiomyopathiesDokument2 Seiten27 Les CardiomyopathiesDoc Odoc100% (1)
- Anglais Examen Et VocDokument54 SeitenAnglais Examen Et VocaliahmadalineNoch keine Bewertungen
- Actinomycose CervicofacialeDokument5 SeitenActinomycose CervicofacialeZineb BelmejdoubNoch keine Bewertungen
- Les Troubles de L'odorat (Ok)Dokument17 SeitenLes Troubles de L'odorat (Ok)EbeNoch keine Bewertungen
- Projet Professionnel Tarmoul Yassine PDFDokument15 SeitenProjet Professionnel Tarmoul Yassine PDFFêt ĤīīNoch keine Bewertungen
- II-234-Diverticulose Colique Et SigmoïditeDokument14 SeitenII-234-Diverticulose Colique Et SigmoïditeNemo LuNoch keine Bewertungen
- Etude PersonnaliseeDokument4 SeitenEtude PersonnaliseeMagib AssureurNoch keine Bewertungen