Das könnte Ihnen auch gefallen
- He Mi Section For Treatment of AnDokument49 SeitenHe Mi Section For Treatment of AnDr.O.R.GANESAMURTHINoch keine Bewertungen
- Healing of Periapical LesionDokument6 SeitenHealing of Periapical LesionRafika Yusniar KurniasariNoch keine Bewertungen
- ParesthesiaoftheupperlipDokument4 SeitenParesthesiaoftheupperlipikeuchi_ogawaNoch keine Bewertungen
- Case Reports Persistent Pain Related To Root Canal Filling and Apical Fenestration: A Case ReportDokument3 SeitenCase Reports Persistent Pain Related To Root Canal Filling and Apical Fenestration: A Case ReportVikas DeepNoch keine Bewertungen
- Overcoming Endodontic Failure with Non-Surgical RetreatmentDokument5 SeitenOvercoming Endodontic Failure with Non-Surgical Retreatmentsharing sessionNoch keine Bewertungen
- Sinus 2 IOSR JDMS PDFDokument3 SeitenSinus 2 IOSR JDMS PDFbhupendraNoch keine Bewertungen
- Saoud 2014Dokument6 SeitenSaoud 2014كرم الباريNoch keine Bewertungen
- Horizontal/oblique Root Fractures in The Palatal Root of Maxillary Molars With Associated Periodontal Destruction: Case ReportsDokument6 SeitenHorizontal/oblique Root Fractures in The Palatal Root of Maxillary Molars With Associated Periodontal Destruction: Case ReportsJuan Pablo BulaciosNoch keine Bewertungen
- A Clinical Approach To Management of TMJ Disorder With Direct Bonding CompositeDokument5 SeitenA Clinical Approach To Management of TMJ Disorder With Direct Bonding Compositewanda oktariaNoch keine Bewertungen
- Case Report/Clinical Technique Nonsurgical Endodontic Treatment of Dens Invaginatus With Large Periradicular Lesion: A CaseDokument4 SeitenCase Report/Clinical Technique Nonsurgical Endodontic Treatment of Dens Invaginatus With Large Periradicular Lesion: A CaseVikas DeepNoch keine Bewertungen
- Gupta2011 PDFDokument5 SeitenGupta2011 PDFAbdul Rahman AlmishhdanyNoch keine Bewertungen
- The Importance of Correct Diagnosis and Treatment in Endo-Periodontal Lesions: A Two Cases ComparisonDokument4 SeitenThe Importance of Correct Diagnosis and Treatment in Endo-Periodontal Lesions: A Two Cases Comparisonedgar curayNoch keine Bewertungen
- Treatment of a Large Maxillary Cyst with Marsupialization and Staged SurgeryDokument8 SeitenTreatment of a Large Maxillary Cyst with Marsupialization and Staged SurgeryDinesh SolankiNoch keine Bewertungen
- Incidence of Post Op Pain After 1 Appointment Endodontic Treatment of Asymptomatic Pulpal Necrosis in Single Rooted Teeth Mulhern 1982Dokument6 SeitenIncidence of Post Op Pain After 1 Appointment Endodontic Treatment of Asymptomatic Pulpal Necrosis in Single Rooted Teeth Mulhern 1982abcder1234Noch keine Bewertungen
- Endodontc Surgical Management of Mucosal FenistrationDokument3 SeitenEndodontc Surgical Management of Mucosal Fenistrationfun timesNoch keine Bewertungen
- Occlusion in Endodontic Management: Cases: Role of Report ofDokument6 SeitenOcclusion in Endodontic Management: Cases: Role of Report ofSophia SaudNoch keine Bewertungen
- A Central Incisor With 4 Independent Root Canals: A Case ReportDokument4 SeitenA Central Incisor With 4 Independent Root Canals: A Case ReportJing XueNoch keine Bewertungen
- Endo024en (065 069) OarDokument5 SeitenEndo024en (065 069) OarNadya PurwantyNoch keine Bewertungen
- PeriapikalDokument7 SeitenPeriapikalHanindyaNoorAgusthaNoch keine Bewertungen
- Complete Healing of A Large Periapical Lesion Following Conservative Root Canal Treatment in Association With Photodynamic TherapyDokument9 SeitenComplete Healing of A Large Periapical Lesion Following Conservative Root Canal Treatment in Association With Photodynamic TherapyAlina AlexandraNoch keine Bewertungen
- Atypically Grown Large Periradicular Cyst Affecting Adjacent Teeth and Leading To Confounding Diagnosis of Non-Endodontic PathologyDokument10 SeitenAtypically Grown Large Periradicular Cyst Affecting Adjacent Teeth and Leading To Confounding Diagnosis of Non-Endodontic PathologyJorge OrbeNoch keine Bewertungen
- Bornstein 2008Dokument5 SeitenBornstein 2008Jing XueNoch keine Bewertungen
- Crim Dentistry2012-525364Dokument6 SeitenCrim Dentistry2012-525364R RahmadaniNoch keine Bewertungen
- Hemisection of A Severely Decayed Mandibular Molar: A Case ReportDokument4 SeitenHemisection of A Severely Decayed Mandibular Molar: A Case Reportkartika tiaraNoch keine Bewertungen
- Fibrous Dysplasia of The Anterior Mandible A Rare HDokument6 SeitenFibrous Dysplasia of The Anterior Mandible A Rare HyesikaichaaNoch keine Bewertungen
- Periapical Cemento-Osseous Dysplasia Case ReportDokument13 SeitenPeriapical Cemento-Osseous Dysplasia Case ReportDha Dina SevofrationNoch keine Bewertungen
- YudzDokument10 SeitenYudzyudisNoch keine Bewertungen
- Ricucci 2014Dokument7 SeitenRicucci 2014leiliromualdoNoch keine Bewertungen
- Daring Occlusal Adjusment (Oa)Dokument9 SeitenDaring Occlusal Adjusment (Oa)Arlanda Diane MahendraNoch keine Bewertungen
- Periapical GranulomaDokument6 SeitenPeriapical GranulomaEzza RiezaNoch keine Bewertungen
- Nance Palatal Arch A Cautionary TaleDokument5 SeitenNance Palatal Arch A Cautionary TaleLanaNoch keine Bewertungen
- HaseebaK EtalDokument5 SeitenHaseebaK EtalIndah VitasariNoch keine Bewertungen
- InterpretDokument4 SeitenInterpretAdzkia Dheyatika AsriNoch keine Bewertungen
- Dental ReviewDokument5 SeitenDental ReviewUmarsyah AliNoch keine Bewertungen
- Apexogenesis After Initial Root Canal TreatmentDokument8 SeitenApexogenesis After Initial Root Canal TreatmentZita AprilliaNoch keine Bewertungen
- Case Report19Dokument6 SeitenCase Report19irfanaNoch keine Bewertungen
- External Cervical Resorption JC FinalDokument46 SeitenExternal Cervical Resorption JC FinalKomal JadhavNoch keine Bewertungen
- Failures of Root Canal TreatmentDokument77 SeitenFailures of Root Canal Treatmenthardeep kaurNoch keine Bewertungen
- Lateral Incisor With Two RootsDokument6 SeitenLateral Incisor With Two RootsKatiana Lins VidalNoch keine Bewertungen
- Medinform 182Dokument6 SeitenMedinform 182Medinform LtdNoch keine Bewertungen
- EndoDokument3 SeitenEndoJessicaLisaNugrohoNoch keine Bewertungen
- Conservative PresentationDokument14 SeitenConservative PresentationHasan Mohammad ShahiduzzamanNoch keine Bewertungen
- 1 s2.0 S0889540622006552 MainDokument13 Seiten1 s2.0 S0889540622006552 MainMarcos Gómez SosaNoch keine Bewertungen
- Montaño (ENDOPERIOfinals)Dokument9 SeitenMontaño (ENDOPERIOfinals)Colleen MontañoNoch keine Bewertungen
- Ozkan 2008Dokument4 SeitenOzkan 2008aditi jhaveriNoch keine Bewertungen
- Compound OdontomaDokument4 SeitenCompound OdontomaMarcus ValentineNoch keine Bewertungen
- Endodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesDokument5 SeitenEndodontic Treatment of Mandibular Premolars With Complex Anatomy Case SeriesInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Clinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportDokument6 SeitenClinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportIqra KhanNoch keine Bewertungen
- 71-Manuscript File-160-1-10-20170719Dokument6 Seiten71-Manuscript File-160-1-10-20170719sulistiyaNoch keine Bewertungen
- Jurnal 1Dokument4 SeitenJurnal 1Dha Dina SevofrationNoch keine Bewertungen
- Endodontic Management of Taurodontism in Maxillary Molar: A Case ReportDokument4 SeitenEndodontic Management of Taurodontism in Maxillary Molar: A Case ReportMeidi KurniaNoch keine Bewertungen
- Pragnesh D Parmar1 Natwar Singh JBNXKDokument4 SeitenPragnesh D Parmar1 Natwar Singh JBNXKpragnesh parmarNoch keine Bewertungen
- Wigler 2013Dokument3 SeitenWigler 2013Leonardo AmaralNoch keine Bewertungen
- Endodontic Retreatment in Case of Failure: Case ReportDokument3 SeitenEndodontic Retreatment in Case of Failure: Case ReportputriraudatulNoch keine Bewertungen
- Endodontic Emergencies - StyleitalianoDokument5 SeitenEndodontic Emergencies - StyleitalianoDr. Valeriu Anghileanu Zubná ambulanciaNoch keine Bewertungen
- OOOO Ricucci 2000Dokument6 SeitenOOOO Ricucci 2000karlaNoch keine Bewertungen
- Multiple Sites of Pink Spot Resorption in Primary TeethDokument44 SeitenMultiple Sites of Pink Spot Resorption in Primary TeethPrachi MulayNoch keine Bewertungen
- Nonsurgical Management of Periapical Lesion: A Case SeriesDokument6 SeitenNonsurgical Management of Periapical Lesion: A Case SeriesFelyciaNoch keine Bewertungen
- Brighter Futures - Orthodontic Endodontic Considerations Part 2Dokument4 SeitenBrighter Futures - Orthodontic Endodontic Considerations Part 2Valonia IreneNoch keine Bewertungen
- Avoiding and Treating Dental Complications: Best Practices in DentistryVon EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieNoch keine Bewertungen
- Frank 2000Dokument10 SeitenFrank 2000magus davilaNoch keine Bewertungen
- Debra Hall Fisher ResumeDokument4 SeitenDebra Hall Fisher Resumeapi-347999772Noch keine Bewertungen
- 2-104-1483773978-2. Tjprc-Ijpdr-Tooth Supported Mandibular Overdenture A Forgotten ConcepDokument6 Seiten2-104-1483773978-2. Tjprc-Ijpdr-Tooth Supported Mandibular Overdenture A Forgotten ConcepTudor LupesNoch keine Bewertungen
- Protesis Fija Linea de TerminacionDokument15 SeitenProtesis Fija Linea de TerminacionjotapintorNoch keine Bewertungen
- Diagnosing Early Interceptive Orthodontic Problems - Part 1: 2 CE CreditsDokument11 SeitenDiagnosing Early Interceptive Orthodontic Problems - Part 1: 2 CE CreditsVijay Prabu GNoch keine Bewertungen
- Lecture 4, Principles of Cavity Preparation (2) - Outline-HandoutDokument4 SeitenLecture 4, Principles of Cavity Preparation (2) - Outline-HandoutJustDen09Noch keine Bewertungen
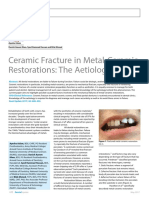
- Ceramic Fracture in Metal-Ceramic Restorations: The AetiologyDokument6 SeitenCeramic Fracture in Metal-Ceramic Restorations: The AetiologyQamar IshfaqueNoch keine Bewertungen
- Seminar on Vertical Maxillo-Mandibular RelationsDokument27 SeitenSeminar on Vertical Maxillo-Mandibular RelationsArun Kumar KVNoch keine Bewertungen
- PART 1 Biologic Basis of PeriodontologyDokument3 SeitenPART 1 Biologic Basis of PeriodontologyNurul HidayatiNoch keine Bewertungen
- 5 Reqs For Occlusal StabilityDokument2 Seiten5 Reqs For Occlusal StabilityNirav MehtaNoch keine Bewertungen
- Pin-Retain For Restoration of Widely Tooth Damaged: Ira WidjiastutiDokument3 SeitenPin-Retain For Restoration of Widely Tooth Damaged: Ira WidjiastutiAngga RanggaNoch keine Bewertungen
- 6 - Occlusion in FPDDokument77 Seiten6 - Occlusion in FPDAnkita Agarwall100% (1)
- Awareness of Bruxism Among Dental StudentsDokument4 SeitenAwareness of Bruxism Among Dental StudentsInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- L3. Apexogenesis - ApexificationDokument44 SeitenL3. Apexogenesis - ApexificationAGENG RAHMA HIJAHANIS ILMASTITI 1Noch keine Bewertungen
- School Dental Health Care Program Receipient Schools Monitoring ToolDokument3 SeitenSchool Dental Health Care Program Receipient Schools Monitoring ToolAnalyn Pedrablanca LanogonNoch keine Bewertungen
- 4964 MMB DentaCare Guide & Terms Levels 2-4Dokument27 Seiten4964 MMB DentaCare Guide & Terms Levels 2-4Jai BhandariNoch keine Bewertungen
- Increasing Vertical DimensionDokument13 SeitenIncreasing Vertical DimensionSiva KumarNoch keine Bewertungen
- 3 Definition and Prevalence of Dentofacial Deformities 2014 Orthognathic SurgeryDokument8 Seiten3 Definition and Prevalence of Dentofacial Deformities 2014 Orthognathic SurgeryiweourvgiuNoch keine Bewertungen
- Exodontia Practice: A Guide to Tooth Extraction InstrumentsDokument148 SeitenExodontia Practice: A Guide to Tooth Extraction InstrumentsnovonetunoNoch keine Bewertungen
- Chapter 11 Occlusal Adjustment PDFDokument8 SeitenChapter 11 Occlusal Adjustment PDFDavid ColonNoch keine Bewertungen
- 11IJDEJul Sep2017Dokument45 Seiten11IJDEJul Sep2017Yady S. Londoño L.Noch keine Bewertungen
- SDCEP MADP Consultation DraftDokument58 SeitenSDCEP MADP Consultation DraftLisa Pramitha SNoch keine Bewertungen
- Minimally Invasive Surgical Techniques-Part 1Dokument69 SeitenMinimally Invasive Surgical Techniques-Part 1Dr. Pragyan SwainNoch keine Bewertungen
- Launch of Close Up Mouth WashDokument28 SeitenLaunch of Close Up Mouth Washrishi2360% (1)
- Classification of Skeletal and Dental Malocclusion: RevisitedDokument8 SeitenClassification of Skeletal and Dental Malocclusion: RevisitedIoana LazarNoch keine Bewertungen
- Sem 15 Occ Eq FinalDokument64 SeitenSem 15 Occ Eq FinalpriyaNoch keine Bewertungen
- Penetration Depth of Irrigants Into Root Dentine After Sonic, Ultrasonic and Photoacoustic ActivationDokument8 SeitenPenetration Depth of Irrigants Into Root Dentine After Sonic, Ultrasonic and Photoacoustic ActivationAndras KuthiNoch keine Bewertungen
- Clinical Assessment New AtientDokument6 SeitenClinical Assessment New AtientLoredana Radu50% (2)
- Lee 2011 Tooth Wear InvestigationDokument9 SeitenLee 2011 Tooth Wear InvestigationKenneth YungNoch keine Bewertungen
- Pharmaceutical Inorganic Chemistry: Unit 3, Chapter 5: Dental Products ScopeDokument1 SeitePharmaceutical Inorganic Chemistry: Unit 3, Chapter 5: Dental Products ScopeHanz Zrhyzer CallaNoch keine Bewertungen