Das könnte Ihnen auch gefallen
- Antepartum ConceptsDokument4 SeitenAntepartum ConceptsKevin VillaranteNoch keine Bewertungen
- BSM M104 Curriculum OutlineDokument3 SeitenBSM M104 Curriculum OutlineDamaris Pandora Songcal0% (1)
- MCN OB Nursing February 22 2021Dokument12 SeitenMCN OB Nursing February 22 2021Kristel Grace OgtipNoch keine Bewertungen
- Sample Letter Templates (4th Year)Dokument49 SeitenSample Letter Templates (4th Year)Yna LafuenteNoch keine Bewertungen
- Lecture Objectives & OutlinesDokument25 SeitenLecture Objectives & OutlinesFelmerPolancoRodaNoch keine Bewertungen
- Care of Mother, Child, Family and Population Group At-Risk or With Problems By: Leani G. BongayonDokument5 SeitenCare of Mother, Child, Family and Population Group At-Risk or With Problems By: Leani G. BongayonChrizelle Esperanzate FlorentinoNoch keine Bewertungen
- Unit 6 - : Reproductive System Test BankDokument10 SeitenUnit 6 - : Reproductive System Test Bankjayrald cruzada100% (1)
- RNC Content and Study GuideDokument11 SeitenRNC Content and Study GuideNicole CanadaNoch keine Bewertungen
- Abnormal PuerperiumDokument23 SeitenAbnormal PuerperiumLynee OlvianaNoch keine Bewertungen
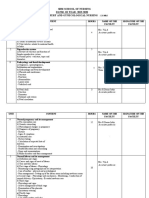
- Teaching Plan 2023-2024Dokument9 SeitenTeaching Plan 2023-2024SANGEETHA RNoch keine Bewertungen
- Elearning Prelim NCM107 2Dokument7 SeitenElearning Prelim NCM107 2HELLE AUBSNoch keine Bewertungen
- Obstetric NursingDokument132 SeitenObstetric NursingSteam LcNoch keine Bewertungen
- EDIZA, RUBY CORAZON - Detailed Lesson PlanDokument10 SeitenEDIZA, RUBY CORAZON - Detailed Lesson PlanRuby Corazon EdizaNoch keine Bewertungen
- OB OutlineDokument3 SeitenOB Outlinejisoo100% (1)
- Maternal NursingDokument130 SeitenMaternal NursingChristine MatasNoch keine Bewertungen
- Lesson Plan On Pregnancy PDFDokument10 SeitenLesson Plan On Pregnancy PDFRuby Corazon EdizaNoch keine Bewertungen
- OBSTETRICS - Midterms - 1.1 - Diagnosis of Pregnancy - TRANSDokument5 SeitenOBSTETRICS - Midterms - 1.1 - Diagnosis of Pregnancy - TRANSAi Gutierrez100% (1)
- Viva ScheduleDokument2 SeitenViva ScheduleToday ViralNoch keine Bewertungen
- Distance Learning Module Flexible: NCM 107ADokument22 SeitenDistance Learning Module Flexible: NCM 107ANurse HoomanNoch keine Bewertungen
- Obstetrics Case Presentation Performa Version 1.5Dokument27 SeitenObstetrics Case Presentation Performa Version 1.5Ajay RajNoch keine Bewertungen
- Pathological Obstetrics, Basic Family Planning and Care of InfantsDokument96 SeitenPathological Obstetrics, Basic Family Planning and Care of InfantsScarlet AmodiaNoch keine Bewertungen
- Human - Anatomy and Physiology 2Dokument2 SeitenHuman - Anatomy and Physiology 2Hermann CHEMEUHINoch keine Bewertungen
- SAP Perawatan Payudara NOVELIADokument10 SeitenSAP Perawatan Payudara NOVELIAOcsiana OxciNoch keine Bewertungen
- B4Y5G3 O - G - With AnswersDokument6 SeitenB4Y5G3 O - G - With AnswersZeke EdgeNoch keine Bewertungen
- Complications of LaborDokument8 SeitenComplications of Laborevangelistakatrina523Noch keine Bewertungen
- NCM 101 (Continuation) Postpartal Period and PediatricsDokument29 SeitenNCM 101 (Continuation) Postpartal Period and PediatricsAudi Kyle SaydovenNoch keine Bewertungen
- Mid 104 ReqDokument3 SeitenMid 104 ReqErika Mae RevadiloNoch keine Bewertungen
- Elearning Ncm107 MidtermDokument9 SeitenElearning Ncm107 MidtermHELLE AUBSNoch keine Bewertungen
- Observational Case Study of A NewbornDokument2 SeitenObservational Case Study of A NewbornCheska Mae PalicNoch keine Bewertungen
- NCM 107j Course Outline Mat PedDokument4 SeitenNCM 107j Course Outline Mat PedHas SimNoch keine Bewertungen
- Physiological and Psychological Changes During PregnancyDokument3 SeitenPhysiological and Psychological Changes During Pregnancykimglaidyl bontuyanNoch keine Bewertungen
- Case Presentation Group CDokument65 SeitenCase Presentation Group CRea Jane Astrologo PastorNoch keine Bewertungen
- Physiologic Changes During Pregnancy: Handout # 7Dokument9 SeitenPhysiologic Changes During Pregnancy: Handout # 7Ram AugustNoch keine Bewertungen
- 1 Anatomy Female Reproductive SystemDokument8 Seiten1 Anatomy Female Reproductive SystemMarwahNoch keine Bewertungen
- Maternity Nursing ReviewDokument52 SeitenMaternity Nursing ReviewDragan Petrovic100% (1)
- Dwnload Full Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions Manual PDFDokument36 SeitenDwnload Full Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions Manual PDFdoughnut.synocilj084s100% (9)
- Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions ManualDokument36 SeitenChildhood and Adolescence Voyages in Development 6th Edition Rathus Solutions Manualaudiblycaribbeeuwiq100% (15)
- Midwifery and Obstetric NursingDokument9 SeitenMidwifery and Obstetric NursingANUM NOORINoch keine Bewertungen
- NCM 107 (OB) Module 1ADokument22 SeitenNCM 107 (OB) Module 1AAmiel simon NgoNoch keine Bewertungen
- Reproduction and Development Study GuideDokument9 SeitenReproduction and Development Study GuidemattvprNoch keine Bewertungen
- Maternal and Child Health Nursing Male Reproductive OrganDokument19 SeitenMaternal and Child Health Nursing Male Reproductive OrganDefensor Pison GringgoNoch keine Bewertungen
- Dwnload Full Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manual PDFDokument36 SeitenDwnload Full Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manual PDFgreeningquinovic25yn2100% (12)
- Full Download Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions ManualDokument36 SeitenFull Download Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manualrakicrodwanb100% (28)
- Labor and Delivery Nursing Knowledge & Skills ChecklistDokument4 SeitenLabor and Delivery Nursing Knowledge & Skills Checklistnorthweststaffing100% (4)
- Session #43 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Dokument4 SeitenSession #43 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNoch keine Bewertungen
- VictorDokument12 SeitenVictorTanya SierraNoch keine Bewertungen
- Topic Outline: APR 14, 2021 Dr. Michelle BuelaDokument5 SeitenTopic Outline: APR 14, 2021 Dr. Michelle BuelaSGD5Christine MendozaNoch keine Bewertungen
- TCM Gynecology Syndromes EtiologyDokument12 SeitenTCM Gynecology Syndromes EtiologyGiota StasinopuluNoch keine Bewertungen
- MCN Exam 2 Study Guide - CompleteDokument87 SeitenMCN Exam 2 Study Guide - CompleteColin MacKenzie100% (1)
- Nursing Practice IIDokument9 SeitenNursing Practice IITiffanny BesaNoch keine Bewertungen
- B.ing YenishacDokument3 SeitenB.ing YenishacYenisha CherinaNoch keine Bewertungen
- Newborn ExaminationDokument9 SeitenNewborn Examinationjosephtimbol123Noch keine Bewertungen
- Childhood and Adolescence Voyages in Development 6th Edition Rathus Solutions ManualDokument12 SeitenChildhood and Adolescence Voyages in Development 6th Edition Rathus Solutions ManualJenniferAguilarrfiax100% (10)
- Family Planning & The Human Reproductive SystemDokument3 SeitenFamily Planning & The Human Reproductive SystemEchuserang FrogletNoch keine Bewertungen
- Supplemental Notes in Maternal Bullets Family PlanningDokument3 SeitenSupplemental Notes in Maternal Bullets Family Planningjohn paul richard mindanaoNoch keine Bewertungen
- Module 5 Case Study PresentationDokument93 SeitenModule 5 Case Study PresentationEDULLANTES ANA MAENoch keine Bewertungen
- Pathological Obstetrics, Basic Family Planning and Care of InfantsDokument95 SeitenPathological Obstetrics, Basic Family Planning and Care of InfantsRhygen Pactol PecoreNoch keine Bewertungen
- Module Introduction and Focus Question (S)Dokument10 SeitenModule Introduction and Focus Question (S)CyrillNoch keine Bewertungen
- Pheromones and Reproduction in MammalsVon EverandPheromones and Reproduction in MammalsJohn VandenberghNoch keine Bewertungen
- Kami Export - Cristina Cotra - Meiosis ActivityDokument7 SeitenKami Export - Cristina Cotra - Meiosis ActivityCristina CotraNoch keine Bewertungen
- Plant Tissue Culture Rajesh BhammarDokument51 SeitenPlant Tissue Culture Rajesh BhammarRajesh Bhammar67% (3)
- EOC Review 5 (Ecology, Classification, & Animal Behavior)Dokument6 SeitenEOC Review 5 (Ecology, Classification, & Animal Behavior)ChloeNoch keine Bewertungen
- Callus CultureDokument24 SeitenCallus CultureHabiba Majeed MalikNoch keine Bewertungen
- Chapter 10 Meiosis and Sexual Reproduction: Multiple Choice QuestionsDokument12 SeitenChapter 10 Meiosis and Sexual Reproduction: Multiple Choice Questionsquiet19Noch keine Bewertungen
- Experiment No. 03: To Studdy The Flower Adapted Too Wind and BirdsDokument5 SeitenExperiment No. 03: To Studdy The Flower Adapted Too Wind and BirdsAryan Khode88% (8)
- Vertebrate Development: Biology II: Form and FunctionDokument41 SeitenVertebrate Development: Biology II: Form and FunctionpoovenmoonoosamyNoch keine Bewertungen
- HeredityDokument4 SeitenHeredityneko -samaNoch keine Bewertungen
- Genbio 2 Las Q4 W1Dokument32 SeitenGenbio 2 Las Q4 W1Carmelia Jhan Fate AbrajanoNoch keine Bewertungen
- Xii Botany Notes (Karachi Board)Dokument83 SeitenXii Botany Notes (Karachi Board)Own CreationsNoch keine Bewertungen
- 14 Human Reproduction: SolutionsDokument18 Seiten14 Human Reproduction: SolutionsEkta ManglaniNoch keine Bewertungen
- Sperm Count IncreaseDokument5 SeitenSperm Count Increaseomomom2710Noch keine Bewertungen
- Maternal and Child Nursing 1 Skills Lab Modele s1Dokument3 SeitenMaternal and Child Nursing 1 Skills Lab Modele s1Crystal MaidenNoch keine Bewertungen
- Cytoplasmic Inheritance in Green Algae: Patterns, Mechanisms and Relation To Sex TypeDokument14 SeitenCytoplasmic Inheritance in Green Algae: Patterns, Mechanisms and Relation To Sex TypeMuhammad Thoriqul FirdausNoch keine Bewertungen
- 2 Introduction To Embryology and FetalDokument55 Seiten2 Introduction To Embryology and Fetaldemeke andebetNoch keine Bewertungen
- SpermiogenesisDokument1 SeiteSpermiogenesispoiwertNoch keine Bewertungen
- Honeymoon Effect Presskit PDFDokument11 SeitenHoneymoon Effect Presskit PDFAnonymous RyHZ0ISas50% (2)
- Human ReproductionDokument16 SeitenHuman ReproductionNajeela khaleelNoch keine Bewertungen
- Physical Structure and Composition of EggsDokument8 SeitenPhysical Structure and Composition of EggsSantos, Glorifhel C.Noch keine Bewertungen
- About The Micropenis ConditionDokument10 SeitenAbout The Micropenis ConditionMicro JackNoch keine Bewertungen
- AQA Biology GCSE Combined B2 Practice AnswersDokument2 SeitenAQA Biology GCSE Combined B2 Practice AnswersMahebul MazidNoch keine Bewertungen
- Introduction To EmbryologyDokument3 SeitenIntroduction To EmbryologyDr Md Abedur Rahman100% (3)
- How Do Organisms Reproduce PDFDokument25 SeitenHow Do Organisms Reproduce PDFBala VisaNoch keine Bewertungen
- Shotgun Fungus LabDokument6 SeitenShotgun Fungus LabSuleiman DaudaNoch keine Bewertungen
- Multiple pregNANCYDokument83 SeitenMultiple pregNANCYDoc RaymondNoch keine Bewertungen
- MenarcheDokument7 SeitenMenarcheBlessing IkangNoch keine Bewertungen
- Name: - Score: - School: - DateDokument14 SeitenName: - Score: - School: - DateELLEN B.SINAHONNoch keine Bewertungen
- Frog Its Reproduct 00 R UghDokument360 SeitenFrog Its Reproduct 00 R UghAlissandra OcampoNoch keine Bewertungen
- Maternal & Child Health Nursing Flashcards QuizletDokument1 SeiteMaternal & Child Health Nursing Flashcards QuizletJosh PagnamitanNoch keine Bewertungen
- Camel Reproduction Some FactsDokument72 SeitenCamel Reproduction Some FactsGovind Narayan PurohitNoch keine Bewertungen