Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Cranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Dokument262 SeitenCranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Alvaro RivCalle87% (15)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- List of Anesthesia Library Books PDFDokument3 SeitenList of Anesthesia Library Books PDFcommandityNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 68 Pacifier (Dokument3 Seiten68 Pacifier (Gokull ShautriNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Chapter 06 NeuroDokument22 SeitenChapter 06 NeuroKarla Fralala100% (1)
- Lucifer Is A Latin Word (From The Words Lucem Ferre), Literally Meaning "Light-Bearer", Which inDokument3 SeitenLucifer Is A Latin Word (From The Words Lucem Ferre), Literally Meaning "Light-Bearer", Which inHendry HuangNoch keine Bewertungen
- Medical Equipment ReplacementDokument15 SeitenMedical Equipment Replacementver_at_workNoch keine Bewertungen
- Distraction OsteogenesisDokument28 SeitenDistraction OsteogenesisManika SinghalNoch keine Bewertungen
- Weight-For-Height BOYS: 2 To 5 Years (Z-Scores)Dokument1 SeiteWeight-For-Height BOYS: 2 To 5 Years (Z-Scores)Malisa Lukman100% (1)
- Weight-For-Height BOYS: 2 To 5 Years (Z-Scores)Dokument1 SeiteWeight-For-Height BOYS: 2 To 5 Years (Z-Scores)Malisa Lukman100% (1)
- Evidence-Based Occlusal Management For Temporomandibular DisorderDokument212 SeitenEvidence-Based Occlusal Management For Temporomandibular Disorderp_nps100% (4)
- 2152014141658clinicalmethods 1 PDFDokument10 Seiten2152014141658clinicalmethods 1 PDFKay BristolNoch keine Bewertungen
- Visual Field TestingDokument16 SeitenVisual Field TestingHendry HuangNoch keine Bewertungen
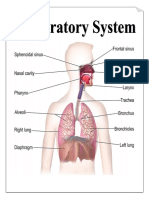
- Parts & Function of Respiratory SystemDokument4 SeitenParts & Function of Respiratory SystemLucille Ballares83% (6)
- Volume/Fluid Responsiveness in The ICUDokument42 SeitenVolume/Fluid Responsiveness in The ICUchadchimaNoch keine Bewertungen
- Rotator Cuff Tear: Nurul Sahida Dina Fadhilah Monika MaghfiraDokument26 SeitenRotator Cuff Tear: Nurul Sahida Dina Fadhilah Monika Maghfiradila_innongNoch keine Bewertungen
- Hematología - Williams (Tomo 1)Dokument1.036 SeitenHematología - Williams (Tomo 1)LIliana100% (3)
- Role For Radiation Therapy in MelanomaDokument13 SeitenRole For Radiation Therapy in MelanomaHendry HuangNoch keine Bewertungen
- Role For Radiation Therapy in MelanomaDokument13 SeitenRole For Radiation Therapy in MelanomaHendry HuangNoch keine Bewertungen
- ChatLog Introduction IPOT X IAT 2020 - 04 - 14 20 - 07Dokument4 SeitenChatLog Introduction IPOT X IAT 2020 - 04 - 14 20 - 07Hendry HuangNoch keine Bewertungen
- Base Excess The BasicsDokument7 SeitenBase Excess The BasicsStaporn KasemsripitakNoch keine Bewertungen
- ChatLog Introduction IPOT X IAT 2020 - 04 - 14 21 - 01Dokument9 SeitenChatLog Introduction IPOT X IAT 2020 - 04 - 14 21 - 01Hendry HuangNoch keine Bewertungen
- Supplementary InformationDokument9 SeitenSupplementary InformationHendry HuangNoch keine Bewertungen
- ChatLog Introduction IPOT X IAT 2020 - 04 - 14 21 - 01Dokument9 SeitenChatLog Introduction IPOT X IAT 2020 - 04 - 14 21 - 01Hendry HuangNoch keine Bewertungen
- ChatLog Q - A IAT Academy 2020 - 05 - 01 16 - 07Dokument3 SeitenChatLog Q - A IAT Academy 2020 - 05 - 01 16 - 07Hendry HuangNoch keine Bewertungen
- Link RISKESDAS 2018Dokument1 SeiteLink RISKESDAS 2018Hendry HuangNoch keine Bewertungen
- New Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For COVID19 PDFDokument32 SeitenNew Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For COVID19 PDFHendry HuangNoch keine Bewertungen
- ChatLog Introduction IPOT X IAT 2020 - 04 - 14 21 - 01Dokument9 SeitenChatLog Introduction IPOT X IAT 2020 - 04 - 14 21 - 01Hendry HuangNoch keine Bewertungen
- Estimation of The Asymptomatic Ratio of Novel Coronavirus Infections COVID19Dokument9 SeitenEstimation of The Asymptomatic Ratio of Novel Coronavirus Infections COVID19Hendry HuangNoch keine Bewertungen
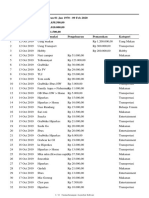
- Laporan - 01 Jan 1970 - 09 Feb 2020 PDFDokument12 SeitenLaporan - 01 Jan 1970 - 09 Feb 2020 PDFHendry HuangNoch keine Bewertungen
- Prolonged Survival in Stage III Melanoma With Ipilimumab Adjuvant TherapyDokument11 SeitenProlonged Survival in Stage III Melanoma With Ipilimumab Adjuvant TherapyIvo AfianiNoch keine Bewertungen
- Webinar Unair Covid 19Dokument73 SeitenWebinar Unair Covid 19Hendry HuangNoch keine Bewertungen
- Demi Download BarangDokument1 SeiteDemi Download BarangHendry HuangNoch keine Bewertungen
- SGA FormDokument2 SeitenSGA Formdwi yuniariNoch keine Bewertungen
- New Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For COVID19 PDFDokument32 SeitenNew Insights On The Antiviral Effects of Chloroquine Against Coronavirus What To Expect For COVID19 PDFHendry HuangNoch keine Bewertungen
- Laporan - 01 Jan - 31 Jan 2020Dokument6 SeitenLaporan - 01 Jan - 31 Jan 2020Hendry HuangNoch keine Bewertungen
- Managing and Administering Medication in Care HomesDokument38 SeitenManaging and Administering Medication in Care HomesHendry Huang100% (1)
- Autism eDokument5 SeitenAutism eHendry HuangNoch keine Bewertungen
- CHT Acfa Boys Z 3 5Dokument1 SeiteCHT Acfa Boys Z 3 5Rivadin NurwanNoch keine Bewertungen
- WHO Growth Chart Boys (Weight For Age) 0-5 YearsDokument1 SeiteWHO Growth Chart Boys (Weight For Age) 0-5 YearsHendry HuangNoch keine Bewertungen
- Gastrointestinal Bleeding in Infants and Children AAPDokument16 SeitenGastrointestinal Bleeding in Infants and Children AAPDina MarselinaNoch keine Bewertungen
- Satisfaction After Restoring Aesthetics and Function in A Child With Amelogenesis Imperfecta: A Case ReportDokument4 SeitenSatisfaction After Restoring Aesthetics and Function in A Child With Amelogenesis Imperfecta: A Case ReportSyifaSahaliyaNoch keine Bewertungen
- Dentistry Semester 1 SAQDokument4 SeitenDentistry Semester 1 SAQKan Chang YuNoch keine Bewertungen
- Medical Incubator 1Dokument6 SeitenMedical Incubator 1Yan YanNoch keine Bewertungen
- Cobas C 311 Brochure Int AgenciesDokument12 SeitenCobas C 311 Brochure Int AgenciesadelNoch keine Bewertungen
- Cynthia Stierman ResumeDokument2 SeitenCynthia Stierman Resumeapi-487498704Noch keine Bewertungen
- Ansiedad y GastritisDokument5 SeitenAnsiedad y Gastritisjose fernandezNoch keine Bewertungen
- A Project ON: Amri Hospital KolkataDokument43 SeitenA Project ON: Amri Hospital KolkataARNAB PANDANoch keine Bewertungen
- Fo1 Barlie Investigation ReportDokument3 SeitenFo1 Barlie Investigation ReportJohn CaezarNoch keine Bewertungen
- Hypersensitivity Rev BWDokument34 SeitenHypersensitivity Rev BWGuhanNoch keine Bewertungen
- Globus PharyngusDokument10 SeitenGlobus PharyngusamalNoch keine Bewertungen
- GBD Lancet Paper 2 Dec 2012Dokument27 SeitenGBD Lancet Paper 2 Dec 2012lawrencehaddadNoch keine Bewertungen
- Domingues-Montanari-2017-Journal of Paediatrics and Child HealthDokument6 SeitenDomingues-Montanari-2017-Journal of Paediatrics and Child Healthmedicina ucnNoch keine Bewertungen
- Challenges To Pediatric ImagingDokument15 SeitenChallenges To Pediatric ImagingKyle GasparNoch keine Bewertungen
- Arterial Blood Gas Values Case Study 2Dokument3 SeitenArterial Blood Gas Values Case Study 2julissaNoch keine Bewertungen
- ClinicalauditDokument41 SeitenClinicalauditAsadulla KhanNoch keine Bewertungen
- TeratomaDokument17 SeitenTeratomaAndri Feisal NasutionNoch keine Bewertungen
- Arjun Reddy (2017) Telugu (Uncensored) - WEB-HD - 1080p - UNTOUCHED - AVC - DD5.1 - 7GB - ESubDokument143 SeitenArjun Reddy (2017) Telugu (Uncensored) - WEB-HD - 1080p - UNTOUCHED - AVC - DD5.1 - 7GB - ESubSentamil SelvanNoch keine Bewertungen