Das könnte Ihnen auch gefallen
- The Predictive Value of Malnutrition For Functional and Cognitive Status in Elderly Hemodialysis PatientsDokument8 SeitenThe Predictive Value of Malnutrition For Functional and Cognitive Status in Elderly Hemodialysis PatientsyafanitaizzatiNoch keine Bewertungen
- REDALYGDokument8 SeitenREDALYGjoel cedeño SánchezNoch keine Bewertungen
- NAD509: Nutrition Assessment: Client HistoryDokument16 SeitenNAD509: Nutrition Assessment: Client HistorySyahrulbariah AbdulhamidNoch keine Bewertungen
- NFPEDokument11 SeitenNFPEpseptinaNoch keine Bewertungen
- Arisawa Et Al, 2014Dokument12 SeitenArisawa Et Al, 2014Jesana LopesNoch keine Bewertungen
- Lec1 Fall23 FSC520 Nutri Assess IntroDokument35 SeitenLec1 Fall23 FSC520 Nutri Assess IntroFatma ZamanNoch keine Bewertungen
- Pediatric Nutrition Assessment Final FarahDokument54 SeitenPediatric Nutrition Assessment Final Farahyuli0% (1)
- Leslie Et Al-2018-European Eating Disorders ReviewDokument10 SeitenLeslie Et Al-2018-European Eating Disorders ReviewGNoch keine Bewertungen
- Prevalence of Eating Disorders Over The 2000-2018 PeriodDokument12 SeitenPrevalence of Eating Disorders Over The 2000-2018 PeriodloloasbNoch keine Bewertungen
- Galmiche 2019 Prevalence EDDokument12 SeitenGalmiche 2019 Prevalence EDCésar BlancoNoch keine Bewertungen
- Prevalence of Eating Disorders Over The 2000-2018 Period: A Systematic Literature ReviewDokument12 SeitenPrevalence of Eating Disorders Over The 2000-2018 Period: A Systematic Literature ReviewRahman FirmansyahNoch keine Bewertungen
- Lec Session 1 and 2Dokument29 SeitenLec Session 1 and 2Elijah EstrellaNoch keine Bewertungen
- Garner 1983Dokument20 SeitenGarner 1983Putri Aurora AngelinaNoch keine Bewertungen
- Protein Energy Malnutrition in CKD PatientsDokument4 SeitenProtein Energy Malnutrition in CKD PatientsEditor IJTSRDNoch keine Bewertungen
- Hajjar Zadeh 2019Dokument8 SeitenHajjar Zadeh 2019TuğbaNoch keine Bewertungen
- 2021 AED Medical Care 4th Ed FINALDokument26 Seiten2021 AED Medical Care 4th Ed FINALSofia GersenowiesNoch keine Bewertungen
- Eating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDokument39 SeitenEating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDylanNoch keine Bewertungen
- Oddy WH, 2018 PDFDokument12 SeitenOddy WH, 2018 PDFAnibal LeNoch keine Bewertungen
- Annals of Medicine and Surgery: SciencedirectDokument3 SeitenAnnals of Medicine and Surgery: SciencedirectAngelica Scherlowski FassulaNoch keine Bewertungen
- Intl J Eating Disorders - 2020 - Hilbert - Psychometric Evaluation of The Eating Disorders in Youth Questionnaire When UsedDokument10 SeitenIntl J Eating Disorders - 2020 - Hilbert - Psychometric Evaluation of The Eating Disorders in Youth Questionnaire When UsedKariena PermanasariNoch keine Bewertungen
- Nursing Care Plan Patient With Diabetes MellitusDokument5 SeitenNursing Care Plan Patient With Diabetes MellitusNajla KhairunnisaNoch keine Bewertungen
- Tayem PDFDokument8 SeitenTayem PDFCynthia MelindaNoch keine Bewertungen
- Nutrition, Health, Diseases: Darmono SSDokument48 SeitenNutrition, Health, Diseases: Darmono SSKiky SuryaNoch keine Bewertungen
- Fnes 368 PresentationDokument13 SeitenFnes 368 Presentationapi-702059884Noch keine Bewertungen
- NCM 114 Lec NotesDokument6 SeitenNCM 114 Lec NotesJustine Claire M. NamocatcatNoch keine Bewertungen
- J of Gastro and Hepatol - 2022 - Bek - Association Between Irritable Bowel Syndrome and Micronutrients A Systematic ReviewDokument13 SeitenJ of Gastro and Hepatol - 2022 - Bek - Association Between Irritable Bowel Syndrome and Micronutrients A Systematic ReviewRaja Alfian IrawanNoch keine Bewertungen
- Eating Disorders in Primary CareDokument13 SeitenEating Disorders in Primary Caresorin.morosan64Noch keine Bewertungen
- Eating Disorders in Children and Adolescents: Nina K. Anderson, and Olivier F. NicolayDokument4 SeitenEating Disorders in Children and Adolescents: Nina K. Anderson, and Olivier F. NicolayParameswaran ManiNoch keine Bewertungen
- Step 2 - ND (New) PDFDokument35 SeitenStep 2 - ND (New) PDFKirito DokkieNoch keine Bewertungen
- Eating Disorders 2016Dokument14 SeitenEating Disorders 2016xxpixiexxNoch keine Bewertungen
- AMERICAN ACADEMY OF PEDIATRICS Identificando e Tratando Transtornos Alimentares InglesDokument10 SeitenAMERICAN ACADEMY OF PEDIATRICS Identificando e Tratando Transtornos Alimentares InglesMarcelo Viana PsiquiatraNoch keine Bewertungen
- Gangguan Makan Pada ObesitasDokument13 SeitenGangguan Makan Pada ObesitasDiaa NagitaaNoch keine Bewertungen
- Association Between Improved Adherence To The JapaDokument8 SeitenAssociation Between Improved Adherence To The JapaFERNANDA MAGDALENA BASTIAS GONZALEZNoch keine Bewertungen
- 1983 Garner EDIDokument22 Seiten1983 Garner EDIAzyan ShahiraNoch keine Bewertungen
- Emotional and Intuitive Eating An Emerging Approach To Eating Behaviours Related To ObesityDokument7 SeitenEmotional and Intuitive Eating An Emerging Approach To Eating Behaviours Related To ObesityferidecelebiNoch keine Bewertungen
- Pilichiewicz 2009Dokument6 SeitenPilichiewicz 2009Stella KwanNoch keine Bewertungen
- Anorexia NervosaDokument12 SeitenAnorexia NervosaDaphney Gracia AntonyNoch keine Bewertungen
- Eating Disorders and Their Implications On Oral Health - Role of DentistsDokument6 SeitenEating Disorders and Their Implications On Oral Health - Role of DentistsThaily MoralesNoch keine Bewertungen
- Diet and Nutrition On MigraineDokument17 SeitenDiet and Nutrition On MigraineRenju KuriakoseNoch keine Bewertungen
- Treatment and Prevention of Childhood Obesity: Sponsored byDokument4 SeitenTreatment and Prevention of Childhood Obesity: Sponsored byThusith WijayawardenaNoch keine Bewertungen
- Jurnal DHR EditDokument35 SeitenJurnal DHR EditMaya Rosmaria PNoch keine Bewertungen
- Who Is at Risk For Nutrition-Related Health Problems?Dokument5 SeitenWho Is at Risk For Nutrition-Related Health Problems?Cler SntsNoch keine Bewertungen
- Ed 277922Dokument147 SeitenEd 277922Yohannes DelesaNoch keine Bewertungen
- The Dietary Inflammatory IndexDokument11 SeitenThe Dietary Inflammatory IndexFrancisco MirettiNoch keine Bewertungen
- Ni Hms 497174Dokument16 SeitenNi Hms 497174nta.gloffkaNoch keine Bewertungen
- Tabel Suplemen EnergyDokument31 SeitenTabel Suplemen EnergySena KawawuraNoch keine Bewertungen
- 1 s2.0 S0165032718328222 MainDokument7 Seiten1 s2.0 S0165032718328222 MainTulaNoch keine Bewertungen
- Effect of Intradialytic Parenteral Nutrition On Quality of Life in Hemodialysis PatientsDokument6 SeitenEffect of Intradialytic Parenteral Nutrition On Quality of Life in Hemodialysis PatientsCarlos Miguel Mendoza LlamocaNoch keine Bewertungen
- Sarc X Con 2Dokument6 SeitenSarc X Con 2Samuel SilvaNoch keine Bewertungen
- Anorexia Myanmar 2019Dokument33 SeitenAnorexia Myanmar 2019Naing LlynNoch keine Bewertungen
- 2nutritionassmt Studay1819Dokument101 Seiten2nutritionassmt Studay1819RaysonChoo100% (2)
- Eating Disorders: Evaluation and Management: Key PointsDokument21 SeitenEating Disorders: Evaluation and Management: Key PointsCassandra BoduchNoch keine Bewertungen
- The Association Between A Nutritional Quality Index and Risk of Chronic DiseaseDokument9 SeitenThe Association Between A Nutritional Quality Index and Risk of Chronic Diseasekamila rodriguezNoch keine Bewertungen
- Validating The Eating Disorder Inventory-2 (EDI-2) in SwedenDokument10 SeitenValidating The Eating Disorder Inventory-2 (EDI-2) in SwedenGiorgioD.KotzalidisNoch keine Bewertungen
- Mental Health Effet 1Dokument21 SeitenMental Health Effet 1Mostafa McheikNoch keine Bewertungen
- Nutrition Care Process (ADIME Process)Dokument15 SeitenNutrition Care Process (ADIME Process)Eizel Nhey G. JADENoch keine Bewertungen
- 20 - BF02982561Dokument5 Seiten20 - BF02982561Giuseppe Peppuz VersariNoch keine Bewertungen
- Mekhancha Dahel2014Dokument1 SeiteMekhancha Dahel2014richard menzNoch keine Bewertungen
- Delaney2014Dokument11 SeitenDelaney2014ryselNoch keine Bewertungen
- Bahan Croup PDFDokument32 SeitenBahan Croup PDFratna ardianaNoch keine Bewertungen
- Guidelines TBC TerbaruDokument160 SeitenGuidelines TBC TerbaruSutoto MoeljadiNoch keine Bewertungen
- Management TB Aafp PDFDokument8 SeitenManagement TB Aafp PDFratna ardianaNoch keine Bewertungen
- Atrioventricular Septal Defect: From Fetus To Adult: Congenital Heart DiseaseDokument7 SeitenAtrioventricular Septal Defect: From Fetus To Adult: Congenital Heart Diseaseratna ardianaNoch keine Bewertungen
- Atrioventricular Septal Defect: From Fetus To Adult: Congenital Heart DiseaseDokument7 SeitenAtrioventricular Septal Defect: From Fetus To Adult: Congenital Heart Diseaseratna ardianaNoch keine Bewertungen
- Cachexia and Protein-Energy Wasting in Children With Chronic Kidney DiseaseDokument9 SeitenCachexia and Protein-Energy Wasting in Children With Chronic Kidney Diseaseratna ardianaNoch keine Bewertungen
- Cachexia and Protein-Energy Wasting in Children With Chronic Kidney DiseaseDokument9 SeitenCachexia and Protein-Energy Wasting in Children With Chronic Kidney Diseaseratna ardianaNoch keine Bewertungen
- School Form 7 (SF7) School Personnel Assignment List and Basic ProfileDokument6 SeitenSchool Form 7 (SF7) School Personnel Assignment List and Basic ProfileMylen Verana MasadingNoch keine Bewertungen
- Dot Net TricksDokument101 SeitenDot Net TrickssathishmnmNoch keine Bewertungen
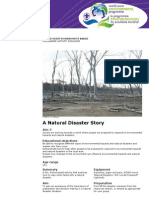
- A Natural Disaster Story: World Scout Environment BadgeDokument4 SeitenA Natural Disaster Story: World Scout Environment BadgeMurali Krishna TNoch keine Bewertungen
- 21st CENTURY LIT (ILOCOS DEITIES)Dokument2 Seiten21st CENTURY LIT (ILOCOS DEITIES)Louise GermaineNoch keine Bewertungen
- Krok 1 Stomatology: Test Items For Licensing ExaminationDokument28 SeitenKrok 1 Stomatology: Test Items For Licensing ExaminationhelloNoch keine Bewertungen
- Synonyms, Antonyms, Spelling CorrectionsDokument10 SeitenSynonyms, Antonyms, Spelling CorrectionsVenkateswara RasupalliNoch keine Bewertungen
- 50 Questions and Answers About Tasawwuf (English) - by Ameer Maulana Akram Awan (MZA)Dokument26 Seiten50 Questions and Answers About Tasawwuf (English) - by Ameer Maulana Akram Awan (MZA)Azim KhanNoch keine Bewertungen
- Risk Management NotesDokument27 SeitenRisk Management NoteskomalNoch keine Bewertungen
- IPTV-Bbc TVP What Is IptvDokument32 SeitenIPTV-Bbc TVP What Is IptvSachin KumarNoch keine Bewertungen
- Indian Entrepreneur Fund PresentationDokument44 SeitenIndian Entrepreneur Fund PresentationHARIHARAN ANoch keine Bewertungen
- Time To Kill PagesDokument24 SeitenTime To Kill PagesFrancisco FerreiraNoch keine Bewertungen
- Inside The Mind of A Master ProcrastinatorDokument5 SeitenInside The Mind of A Master ProcrastinatorDianaNoch keine Bewertungen
- 1927 To 1939 New PDFDokument8 Seiten1927 To 1939 New PDFahmed razaNoch keine Bewertungen
- Note 1-Estate Under AdministrationDokument8 SeitenNote 1-Estate Under AdministrationNur Dina AbsbNoch keine Bewertungen
- The 5 Best 5G Use Cases: Brian SantoDokument4 SeitenThe 5 Best 5G Use Cases: Brian SantoabdulqaderNoch keine Bewertungen
- Code No.: Etit 401 L T C Paper: Advanced Computer Networks 3 1 4Dokument4 SeitenCode No.: Etit 401 L T C Paper: Advanced Computer Networks 3 1 4Han JeeNoch keine Bewertungen
- Section 6 Novation: Study GuideDokument11 SeitenSection 6 Novation: Study GuideElsha DamoloNoch keine Bewertungen
- Wavelets and Signal ProcessingDokument193 SeitenWavelets and Signal ProcessingAlbeno Saleh AhmadNoch keine Bewertungen
- Ad3na0ab (COMBI NACCO-ing)Dokument30 SeitenAd3na0ab (COMBI NACCO-ing)Kaique MelloNoch keine Bewertungen
- Trading With The Heikin Ashi Candlestick OscillatorDokument7 SeitenTrading With The Heikin Ashi Candlestick OscillatorDarren TanNoch keine Bewertungen
- Batch Fed BatchDokument60 SeitenBatch Fed BatchAyesha RalliyaNoch keine Bewertungen
- Karakteristik Padi Gogo Lokal Yang Diber 325acbceDokument10 SeitenKarakteristik Padi Gogo Lokal Yang Diber 325acbcemuhammad arjoniNoch keine Bewertungen
- Against Temple Adverse Possession by Private PersonDokument12 SeitenAgainst Temple Adverse Possession by Private PersonBest NiftyNoch keine Bewertungen
- Current Trends in Teaching and Learning EFLDokument13 SeitenCurrent Trends in Teaching and Learning EFLyimigor100% (1)
- Contoh MOTIVATION LETTERDokument19 SeitenContoh MOTIVATION LETTERDavin Tiska AbrianiNoch keine Bewertungen
- 02 Clemente V CADokument8 Seiten02 Clemente V CAATRNoch keine Bewertungen
- Trinity The Father, The Son and The Holy SpiritDokument3 SeitenTrinity The Father, The Son and The Holy SpiritThomas Lorenz (Fit For Faith Ministries)100% (1)
- Environmental Education Strategy (2010-2014) : United Republic of TanzaniaDokument63 SeitenEnvironmental Education Strategy (2010-2014) : United Republic of Tanzaniaalli sheeranNoch keine Bewertungen
- Sandblasting and Other Air-Based Blasting: Guidance For Generators of Blasting WasteDokument7 SeitenSandblasting and Other Air-Based Blasting: Guidance For Generators of Blasting WasteEarthNav Trading CorporationNoch keine Bewertungen
- AbstractDokument28 SeitenAbstractrobin saxenaNoch keine Bewertungen