Das könnte Ihnen auch gefallen
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentVon EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNoch keine Bewertungen
- Kyphoplasty Vs Vertebral Body StentingDokument8 SeitenKyphoplasty Vs Vertebral Body StentingPankaj VatsaNoch keine Bewertungen
- Anterior Cruciate Ligament Reconstruction: A Practical Surgical GuideVon EverandAnterior Cruciate Ligament Reconstruction: A Practical Surgical GuideNoch keine Bewertungen
- Conferences and Reviews Total Hip Arthroplasty: or An A ReconDokument7 SeitenConferences and Reviews Total Hip Arthroplasty: or An A ReconSekar CitrasariNoch keine Bewertungen
- Rib FractureDokument6 SeitenRib FracturenasyilaputriNoch keine Bewertungen
- The Composite Spreader FlapDokument11 SeitenThe Composite Spreader FlapameliNoch keine Bewertungen
- A 3D Visualization Tool For The Design A PDFDokument11 SeitenA 3D Visualization Tool For The Design A PDFIsabelGuijarroMartinezNoch keine Bewertungen
- Total Shoulder Arthroplasty, An Overview, Indicatins and Prosthetic OptionsDokument4 SeitenTotal Shoulder Arthroplasty, An Overview, Indicatins and Prosthetic OptionsYafiahnaf FirdausNoch keine Bewertungen
- Quadrimalleolar Fractures of The Ankle: Think 360°-A Step-By-Step Guide On Evaluation and FixationDokument3 SeitenQuadrimalleolar Fractures of The Ankle: Think 360°-A Step-By-Step Guide On Evaluation and FixationFRANCISCONoch keine Bewertungen
- Artigo ClamshellDokument15 SeitenArtigo ClamshellbritocirurgiadamaoNoch keine Bewertungen
- 01 MynckeDokument10 Seiten01 MynckeIrina DesyatykhNoch keine Bewertungen
- 10 11607@jomi 8122Dokument8 Seiten10 11607@jomi 8122Marlene Kasumi Gantier TakanoNoch keine Bewertungen
- Solomon 2010Dokument10 SeitenSolomon 2010Roger WatersNoch keine Bewertungen
- Reconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyDokument9 SeitenReconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyNorin FornaNoch keine Bewertungen
- Acetabular Reconstruction in Total Hip Arthroplasty: EditorialDokument14 SeitenAcetabular Reconstruction in Total Hip Arthroplasty: Editorialana starcevicNoch keine Bewertungen
- Surgical Challenges in Complex Primary Total Hip ADokument9 SeitenSurgical Challenges in Complex Primary Total Hip Aehabede6445Noch keine Bewertungen
- Efect of Two Types of Shoulder Prosthesis On The Muscle Forces Using A Generic Multibody Model For Diferent Arm MotionsDokument19 SeitenEfect of Two Types of Shoulder Prosthesis On The Muscle Forces Using A Generic Multibody Model For Diferent Arm MotionsOussama El B'charriNoch keine Bewertungen
- True Ponte Osteotomy Ponte 2018Dokument10 SeitenTrue Ponte Osteotomy Ponte 2018Azmi FarhadiNoch keine Bewertungen
- Microsoft Word - THR Preprint - Thr+PreprintDokument2 SeitenMicrosoft Word - THR Preprint - Thr+PreprintNuno GueiralNoch keine Bewertungen
- Chapter 19Dokument25 SeitenChapter 19MuhammadMusa47Noch keine Bewertungen
- Optimizing Stability in Distal Humeral Fracture Fixation: Historical PerspectiveDokument9 SeitenOptimizing Stability in Distal Humeral Fracture Fixation: Historical PerspectiveNazir KhanNoch keine Bewertungen
- Avn OrtoDokument3 SeitenAvn OrtoandikaNoch keine Bewertungen
- Deen 2017Dokument5 SeitenDeen 2017GERARDO TORRES RUIZNoch keine Bewertungen
- Ongoing Debate in Orbital FracturesDokument11 SeitenOngoing Debate in Orbital Fractureslaljadeff12100% (1)
- Acetabular Component PositioningDokument4 SeitenAcetabular Component PositioningPurushotham NalamatiNoch keine Bewertungen
- Orthopaedics & Traumatology: Surgery & ResearchDokument5 SeitenOrthopaedics & Traumatology: Surgery & ResearchMohan DesaiNoch keine Bewertungen
- Costochondral GraftsDokument5 SeitenCostochondral Graftssmartdoc36100% (1)
- FulltextDokument10 SeitenFulltextDenis AlexandruNoch keine Bewertungen
- Management of Complex Orbital Fractures: Article in PressDokument5 SeitenManagement of Complex Orbital Fractures: Article in Pressstoia_sebiNoch keine Bewertungen
- 1.a) Structure:: Fibrocartilaginous Knee Tibia Femur Fossae CondylesDokument11 Seiten1.a) Structure:: Fibrocartilaginous Knee Tibia Femur Fossae CondylesWaiKheongNoch keine Bewertungen
- AC Plate On The Treatment of Fractures and Dislocation of Acromio-Clavicular Joint. J. Schmidt, A. WittDokument20 SeitenAC Plate On The Treatment of Fractures and Dislocation of Acromio-Clavicular Joint. J. Schmidt, A. WittNuno Craveiro LopesNoch keine Bewertungen
- Guidedboneregeneration Inalveolarbone Reconstruction: Istvan A. Urban,, Alberto MonjeDokument8 SeitenGuidedboneregeneration Inalveolarbone Reconstruction: Istvan A. Urban,, Alberto MonjeVanessa Iñiguez ArmijosNoch keine Bewertungen
- Anatomic Double BundleDokument8 SeitenAnatomic Double BundleVijay KumarNoch keine Bewertungen
- Orthopaedic Surgery - 2022 - Bota - Complex Functional Posttraumatic Shoulder Reconstruction Using Shoulder ArthroplastyDokument6 SeitenOrthopaedic Surgery - 2022 - Bota - Complex Functional Posttraumatic Shoulder Reconstruction Using Shoulder ArthroplastyOli BotaNoch keine Bewertungen
- Distal Humeral Fractures-Current Concepts PDFDokument11 SeitenDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNoch keine Bewertungen
- Orthopaedic Surgery - 2023 - Ying - Treatment of Acetabular Bone Defect in Revision of Total Hip Arthroplasty Using 3DDokument8 SeitenOrthopaedic Surgery - 2023 - Ying - Treatment of Acetabular Bone Defect in Revision of Total Hip Arthroplasty Using 3DOnSolomonNoch keine Bewertungen
- Proyeccion Hombro BenageaunDokument3 SeitenProyeccion Hombro Benageaunherytz martinez gomezNoch keine Bewertungen
- Management of Cubitus Varus Deformity in Children by Closed Dome OsteotomyDokument5 SeitenManagement of Cubitus Varus Deformity in Children by Closed Dome OsteotomyPiyush W GadegoneNoch keine Bewertungen
- 2023 - Mechanical Characterization of A NovelDokument9 Seiten2023 - Mechanical Characterization of A NovelAbdelrahman AbdelgawadNoch keine Bewertungen
- Placa Cervical Anterior AtlantisDokument39 SeitenPlaca Cervical Anterior AtlantisJavier Peña ChavezNoch keine Bewertungen
- 2023 Article 181Dokument8 Seiten2023 Article 181Deborah SalinasNoch keine Bewertungen
- 03 de RoeckDokument5 Seiten03 de RoeckAntonio FagaNoch keine Bewertungen
- Niki 2015Dokument5 SeitenNiki 2015andreicorni25Noch keine Bewertungen
- Brace Modifications That Can Result in Improved Curve Correction in Idiopathic ScoliosisDokument7 SeitenBrace Modifications That Can Result in Improved Curve Correction in Idiopathic ScoliosisjeanNoch keine Bewertungen
- Dual Mobility Cups For Total Hip ArthroplastyDokument11 SeitenDual Mobility Cups For Total Hip ArthroplastyhardboneNoch keine Bewertungen
- Functional and Cosmetic Outcome After Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) With and Without The Support of 3D-PrintedDokument12 SeitenFunctional and Cosmetic Outcome After Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) With and Without The Support of 3D-PrintedDoruk OrgunNoch keine Bewertungen
- Treatment of Femoral Neck Fractures in Elderly Patients Over 60 Years of Age - Which Is The Ideal Modality of Primary Joint Replacement?Dokument8 SeitenTreatment of Femoral Neck Fractures in Elderly Patients Over 60 Years of Age - Which Is The Ideal Modality of Primary Joint Replacement?FakhriMuhamadRizaldiNoch keine Bewertungen
- Cope Land Op TechDokument24 SeitenCope Land Op Techsiddig7Noch keine Bewertungen
- Scoliosis BraceDokument8 SeitenScoliosis BraceChandralina PakpahanNoch keine Bewertungen
- Chilean Radiology MagazineDokument34 SeitenChilean Radiology MagazineJorge A. Prado BrangoNoch keine Bewertungen
- Osteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingDokument5 SeitenOsteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingAnonymous Qt31LLO1lNoch keine Bewertungen
- Knee MobilebearingkneeDokument20 SeitenKnee MobilebearingkneeJobin VargheseNoch keine Bewertungen
- LCP Inlay Tibial SPORTMEDARTHRO 2020Dokument4 SeitenLCP Inlay Tibial SPORTMEDARTHRO 2020orthopaedicsUV martNoch keine Bewertungen
- jkhs-21-202 Ko enDokument9 Seitenjkhs-21-202 Ko enlaurenNoch keine Bewertungen
- OUtcome After Limted or Extensive BursectomyDokument8 SeitenOUtcome After Limted or Extensive BursectomySeno adipNoch keine Bewertungen
- Spinal Pedicle Subtraction Osteotomy For Fixed Sagittal Imbalance Patients. Hyun 2013Dokument8 SeitenSpinal Pedicle Subtraction Osteotomy For Fixed Sagittal Imbalance Patients. Hyun 2013Arsène NtiniNoch keine Bewertungen
- Current Trends Rhinoplasty Rollin DDokument7 SeitenCurrent Trends Rhinoplasty Rollin Dmaxillo.arrasNoch keine Bewertungen
- Total Elbow TechniqueDokument7 SeitenTotal Elbow Techniquedidit satmokoNoch keine Bewertungen
- Cuñas MetalicasDokument8 SeitenCuñas MetalicasOciel AcostaNoch keine Bewertungen
- 10 1016@j Jos 2016 04 015Dokument7 Seiten10 1016@j Jos 2016 04 015osmann52Noch keine Bewertungen
- SOP AP Herpes ZosterDokument1 SeiteSOP AP Herpes ZosterSilma FarrahaNoch keine Bewertungen
- SOP AP DyspepsiaDokument1 SeiteSOP AP DyspepsiaSilma FarrahaNoch keine Bewertungen
- SOP AP Asma BronkhialDokument1 SeiteSOP AP Asma BronkhialSilma FarrahaNoch keine Bewertungen
- Pediatric Spine MRI: Occult Spinal DysraphismsDokument5 SeitenPediatric Spine MRI: Occult Spinal DysraphismsSilma FarrahaNoch keine Bewertungen
- Classification of Adolescent Idiopathic ScoliosisDokument4 SeitenClassification of Adolescent Idiopathic ScoliosisBangkit PrimayudhaNoch keine Bewertungen
- Classification of Adolescent Idiopathic ScoliosisDokument60 SeitenClassification of Adolescent Idiopathic ScoliosisSilma FarrahaNoch keine Bewertungen
- Classification of Adolescent Idiopathic ScoliosisDokument4 SeitenClassification of Adolescent Idiopathic ScoliosisBangkit PrimayudhaNoch keine Bewertungen
- Psikiatri 2Dokument1 SeitePsikiatri 2Silma FarrahaNoch keine Bewertungen
- 1Dokument1 Seite1Silma FarrahaNoch keine Bewertungen
- ScoliosisDokument10 SeitenScoliosisSilma FarrahaNoch keine Bewertungen
- PsikiatriDokument1 SeitePsikiatriSilma FarrahaNoch keine Bewertungen
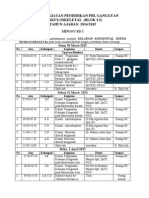
- Jadwal Kuliah Blok 3.5 2015Dokument12 SeitenJadwal Kuliah Blok 3.5 2015Silma FarrahaNoch keine Bewertungen
- Clinical Presentations of Cutaneous Tuberculosis: Original ArticleDokument3 SeitenClinical Presentations of Cutaneous Tuberculosis: Original ArticleSilma FarrahaNoch keine Bewertungen
- Scoliosis PDFDokument19 SeitenScoliosis PDFdallas100% (1)
- Jadwal Skill Lab 3.3Dokument13 SeitenJadwal Skill Lab 3.3Silma FarrahaNoch keine Bewertungen
- Scoliosis PDFDokument19 SeitenScoliosis PDFdallas100% (1)
- Fimmu 04 00507 PDFDokument20 SeitenFimmu 04 00507 PDFSilma FarrahaNoch keine Bewertungen
- Mode of InjuryDokument48 SeitenMode of InjuryirfanzukriNoch keine Bewertungen
- Alveolar Bone QuestionsDokument9 SeitenAlveolar Bone QuestionsCzar Martinez0% (1)
- A Radiologist's Guide To: Wrist AlignmentDokument35 SeitenA Radiologist's Guide To: Wrist Alignmentsisiramohan100% (1)
- Intro To Diagnostic Imaging - 2 - Prof - Dr.i̇smet TAMERDokument37 SeitenIntro To Diagnostic Imaging - 2 - Prof - Dr.i̇smet TAMERAly MssreNoch keine Bewertungen
- Cazuri-ColoanapptDokument69 SeitenCazuri-ColoanapptmiravoineaNoch keine Bewertungen
- Spine TraumaDokument52 SeitenSpine Traumaapi-26159412100% (1)
- Selamat Pagi Dokter BTKV 14-07-2022Dokument9 SeitenSelamat Pagi Dokter BTKV 14-07-2022Arif KurniawanNoch keine Bewertungen
- Medicine: Hoffa Fracture of The Femoral CondyleDokument7 SeitenMedicine: Hoffa Fracture of The Femoral Condylesheshagiri vNoch keine Bewertungen
- Musculoskeletal RadiologyDokument5 SeitenMusculoskeletal Radiologyapi-3743483Noch keine Bewertungen
- Aos A1poster UpperCervCS Mar18Dokument1 SeiteAos A1poster UpperCervCS Mar18Aussie AuliaNoch keine Bewertungen
- NCM 104 Musculo Anaphy, DxticsDokument80 SeitenNCM 104 Musculo Anaphy, DxticsJordz PlaciNoch keine Bewertungen
- Cervical Spine FracturesDokument58 SeitenCervical Spine Fracturesamarsidin1Noch keine Bewertungen
- Skeletal SystemDokument23 SeitenSkeletal SystemNickmor OamlinNoch keine Bewertungen
- Bone DensityDokument18 SeitenBone Densitydhwanit31100% (1)
- MCQ Tutor in Radiology FRCR Part 1 PDFDokument121 SeitenMCQ Tutor in Radiology FRCR Part 1 PDFSharifa Abdulghaffar70% (10)
- Osteoid OsteomaDokument6 SeitenOsteoid OsteomadrkaushikduttaNoch keine Bewertungen
- Jenisie Pasigan - Ch. 8-2 - Skeletal System Notes Packet (Part II)Dokument5 SeitenJenisie Pasigan - Ch. 8-2 - Skeletal System Notes Packet (Part II)Jenisie PasiganNoch keine Bewertungen
- The Growth of The MandibleDokument43 SeitenThe Growth of The MandibleSusie FahimNoch keine Bewertungen
- Injuries of Wrist and HandDokument34 SeitenInjuries of Wrist and HandMugunthan Rangiah100% (1)
- Liceo de Cagayan University: WorksheetDokument7 SeitenLiceo de Cagayan University: WorksheetLol lolNoch keine Bewertungen
- Ethan McDaniel - Skeletal System Study GuideDokument7 SeitenEthan McDaniel - Skeletal System Study GuideJohn BroNoch keine Bewertungen
- Crif PDFDokument3 SeitenCrif PDFIqbal BaryarNoch keine Bewertungen
- Acetabulum Fractures - Classification and Management - Emile LetournelDokument26 SeitenAcetabulum Fractures - Classification and Management - Emile LetournelThanat AuwattanamongkolNoch keine Bewertungen
- Ocular Anatomy and Physiology: Myra Obcena - de Leon, Od Clinical Coordinator Davao Doctors CollegeDokument60 SeitenOcular Anatomy and Physiology: Myra Obcena - de Leon, Od Clinical Coordinator Davao Doctors CollegeLezahbef Neaj SollogonNoch keine Bewertungen
- Bone Bruising and Bone Marrow Edema SyndromesDokument8 SeitenBone Bruising and Bone Marrow Edema SyndromesRekkiNoch keine Bewertungen
- Complete Guide To Abdominal TrainingDokument223 SeitenComplete Guide To Abdominal TrainingLynseyNoch keine Bewertungen
- Fractures of The Scapula: Charles D. NewtonDokument12 SeitenFractures of The Scapula: Charles D. NewtonasheneyNoch keine Bewertungen
- Anatomy and Physiology of The Nose and Paranasal SinusesDokument2 SeitenAnatomy and Physiology of The Nose and Paranasal SinusesNuardi YusufNoch keine Bewertungen
- Ulna (Bone and Attachments) Flow ChartDokument2 SeitenUlna (Bone and Attachments) Flow ChartNicoleta PSNoch keine Bewertungen
- Surface & Radiological Anatomy (3rd Ed) (Gnv64)Dokument226 SeitenSurface & Radiological Anatomy (3rd Ed) (Gnv64)Sllavko K. Kallfa100% (4)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Von EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Bewertung: 5 von 5 Sternen5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerVon EverandGut: the new and revised Sunday Times bestsellerBewertung: 4 von 5 Sternen4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (378)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (58)