Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- OSCE Qs Internal MedicineDokument29 SeitenOSCE Qs Internal MedicineRancesh FamoNoch keine Bewertungen
- Percutaneous Interventions ExplainedDokument55 SeitenPercutaneous Interventions ExplainedShannon Bellamy-FoggNoch keine Bewertungen
- Updates American Heart Association Cardiopulmonary Resuscitation GuidelineDokument32 SeitenUpdates American Heart Association Cardiopulmonary Resuscitation GuidelineramzishindiNoch keine Bewertungen
- Biol 2301 - Unit 8 - Circulation StudentDokument82 SeitenBiol 2301 - Unit 8 - Circulation Studentapi-664744800Noch keine Bewertungen
- Jurnal 3Dokument4 SeitenJurnal 3Arum RaniNoch keine Bewertungen
- Cicrulatory and Immune Workbook KEYDokument32 SeitenCicrulatory and Immune Workbook KEYgeorgia robinsonNoch keine Bewertungen
- Definition of Dread DiseasesDokument4 SeitenDefinition of Dread Diseaseslancekim21Noch keine Bewertungen
- 2023 Atrial Fibrillation Guideline-at-a-Glance: Societal StatementDokument5 Seiten2023 Atrial Fibrillation Guideline-at-a-Glance: Societal StatementMiguel Limaylla ZapataNoch keine Bewertungen
- ACT 4 Scene 1 - HypertensionDokument32 SeitenACT 4 Scene 1 - Hypertensionsameersidana18Noch keine Bewertungen
- DR Sandeep - EISENMENGER SYNDROMEDokument81 SeitenDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNoch keine Bewertungen
- ABC of Clinical Electrocardiography Atrial ArrhythmiasDokument6 SeitenABC of Clinical Electrocardiography Atrial ArrhythmiasIgnacio Aguilar ValdiviesoNoch keine Bewertungen
- Stress Echocardiography: Dr. Surinder Singh HansraDokument35 SeitenStress Echocardiography: Dr. Surinder Singh HansrasshansraNoch keine Bewertungen
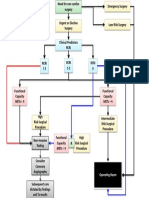
- Cardiac Risk Assessemnt FlowchartDokument1 SeiteCardiac Risk Assessemnt FlowchartjamesomooreNoch keine Bewertungen
- Hypertension PathophysiologyDokument1 SeiteHypertension PathophysiologyTiffany Blanca Evangelista RaiNoch keine Bewertungen
- Amity College of Nursing: Nursing Care Plan ON Heart FailureDokument20 SeitenAmity College of Nursing: Nursing Care Plan ON Heart Failurejyoti puniaNoch keine Bewertungen
- ALS Recertification CourseDokument64 SeitenALS Recertification CoursePanagiotis Iliopoulos100% (1)
- Del Nido Article MaterialDokument41 SeitenDel Nido Article Materialzaigham khalidNoch keine Bewertungen
- Pena Medika: ISSN: 2086-843XDokument19 SeitenPena Medika: ISSN: 2086-843XNurul FitriaNoch keine Bewertungen
- Cardiovascular Clinical ExaminationDokument27 SeitenCardiovascular Clinical ExaminationAshiniNoch keine Bewertungen
- Systolic and Diastolic Blood Pressure, Pulse Pressure, and Mean Arterial Pressure As Predictors of Cardiovascular Disease Risk in MenDokument8 SeitenSystolic and Diastolic Blood Pressure, Pulse Pressure, and Mean Arterial Pressure As Predictors of Cardiovascular Disease Risk in MenSebastian Tabares RodriguezNoch keine Bewertungen
- Acls Drug OverviewDokument2 SeitenAcls Drug OverviewBruce Abramowitz100% (1)
- Cardio Vascular System NursingDokument2 SeitenCardio Vascular System NursingGade BalajiNoch keine Bewertungen
- 200L FON PRESENTATION Group 1Dokument13 Seiten200L FON PRESENTATION Group 1jonaNoch keine Bewertungen
- Metoprolol to Tenecteplase Cardiac Drug GuideDokument5 SeitenMetoprolol to Tenecteplase Cardiac Drug GuideGilbert NeahNoch keine Bewertungen
- Cardiologist in Pimpri, WakadDokument6 SeitenCardiologist in Pimpri, Wakadsachin hundekariNoch keine Bewertungen
- Newlife AEDDokument8 SeitenNewlife AEDRoger PerezNoch keine Bewertungen
- ABPI-Ankle Brachial Pressure IndexDokument23 SeitenABPI-Ankle Brachial Pressure IndexTamsi MahiNoch keine Bewertungen
- Dual Antiplatelet Therapy Benefits for Prior MI PatientsDokument40 SeitenDual Antiplatelet Therapy Benefits for Prior MI PatientsKarren Taquiqui PleteNoch keine Bewertungen
- Pulmonary EmbolismDokument3 SeitenPulmonary EmbolismdeanneadrianoNoch keine Bewertungen
- Abdominal Aortic Aneurysm 1Dokument44 SeitenAbdominal Aortic Aneurysm 1Kendy Rizky Hadyan100% (1)