Das könnte Ihnen auch gefallen
- Breast Cancer PathophysiologyDokument2 SeitenBreast Cancer PathophysiologyErba100% (7)
- John Jameson, Danny Bryden - Care of The Critically Ill Surgical Patient Student Handbook-The Royal College of Surgeons of England (2017)Dokument355 SeitenJohn Jameson, Danny Bryden - Care of The Critically Ill Surgical Patient Student Handbook-The Royal College of Surgeons of England (2017)osamaeNoch keine Bewertungen
- PIIS0031302518304471Dokument1 SeitePIIS0031302518304471John LêNoch keine Bewertungen
- CA Treatment Osteosarcoma Pedi Web AlgorithmDokument6 SeitenCA Treatment Osteosarcoma Pedi Web AlgorithmyaseenNoch keine Bewertungen
- Ca Treatment Rectal Web AlgorithmDokument17 SeitenCa Treatment Rectal Web AlgorithmPatrick JohnNoch keine Bewertungen
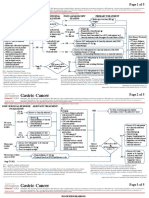
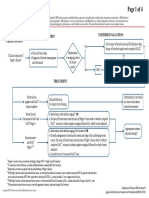
- Ca Treatment Gastric Web AlgorithmDokument5 SeitenCa Treatment Gastric Web AlgorithmEVELYN EZEKWENoch keine Bewertungen
- Ca Treatment Prostate Web AlgorithmDokument12 SeitenCa Treatment Prostate Web AlgorithmCalvinNoch keine Bewertungen
- Ca - Treatment-Breast-Inflammatory-Web-AlgorithmDokument19 SeitenCa - Treatment-Breast-Inflammatory-Web-AlgorithmAgustin SierraNoch keine Bewertungen
- Enfermedad de PagetDokument4 SeitenEnfermedad de PagetNicolás BertachiniNoch keine Bewertungen
- Cancer de Mama y EmbarazoDokument5 SeitenCancer de Mama y EmbarazoNicolás BertachiniNoch keine Bewertungen
- CA Treatment Small Cell Web AlgorithmDokument8 SeitenCA Treatment Small Cell Web AlgorithmbharatNoch keine Bewertungen
- CA Treatment Leptomeningeal Web AlgorithmDokument5 SeitenCA Treatment Leptomeningeal Web Algorithmsugoiman100% (1)
- Ca Treatment Paget S Web AlgorithmDokument4 SeitenCa Treatment Paget S Web AlgorithmAgustin SierraNoch keine Bewertungen
- Ca Treatment Breast Noninvasive Web AlgorithmDokument8 SeitenCa Treatment Breast Noninvasive Web AlgorithmAgustin SierraNoch keine Bewertungen
- Ca Treatment Breast Noninvasive Web AlgorithmDokument6 SeitenCa Treatment Breast Noninvasive Web Algorithmmarcelo chavez diazNoch keine Bewertungen
- Ca Treatment Breast Invasive Web AlgorithmDokument27 SeitenCa Treatment Breast Invasive Web AlgorithmAgustin SierraNoch keine Bewertungen
- Cancer of The Endometrium PDFDokument6 SeitenCancer of The Endometrium PDFYanita BetraNoch keine Bewertungen
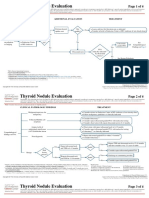
- Clin Management Thyroid Nodule Eval Web AlgorithmDokument4 SeitenClin Management Thyroid Nodule Eval Web AlgorithmMeutia sariNoch keine Bewertungen
- Ca Treatment Phyllodes Web Algorithm PDFDokument4 SeitenCa Treatment Phyllodes Web Algorithm PDFtaufikolingNoch keine Bewertungen
- Clin Management Pacemaker Web AlgorithmDokument8 SeitenClin Management Pacemaker Web AlgorithmRui FonteNoch keine Bewertungen
- Bmjopen 2021 054365 PDFDokument8 SeitenBmjopen 2021 054365 PDFDiego Andrés Bolaños MayaNoch keine Bewertungen
- Surgery PearlsDokument2 SeitenSurgery Pearlspatriciaatan1497Noch keine Bewertungen
- 2020 21 Matrix Covid19 st6 7 Who Switched To 2019 CoreDokument4 Seiten2020 21 Matrix Covid19 st6 7 Who Switched To 2019 CoreOzhenNoch keine Bewertungen
- PRESENTACION Parte3Dokument28 SeitenPRESENTACION Parte3B Mobile T5Noch keine Bewertungen
- Trauma GravidaDokument39 SeitenTrauma Gravidaralucast88Noch keine Bewertungen
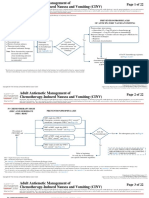
- Page 1 of 22: Risk Assessment Prevention/Prophylaxis of Anticipatory Nausea/VomitingDokument22 SeitenPage 1 of 22: Risk Assessment Prevention/Prophylaxis of Anticipatory Nausea/VomitingEmaNoch keine Bewertungen
- Assessment and Management of Delirium in Pediatric PatientsDokument7 SeitenAssessment and Management of Delirium in Pediatric PatientsEunike Karamoy100% (1)
- CA Treatment Phyllodes Web AlgorithmDokument4 SeitenCA Treatment Phyllodes Web AlgorithmMuhammad SubhiNoch keine Bewertungen
- Protocol Update Dec 2019Dokument13 SeitenProtocol Update Dec 2019Aarzu ChoudharyNoch keine Bewertungen
- Contemporary Management of Acute Pancreatitis: What You Need To KnowDokument10 SeitenContemporary Management of Acute Pancreatitis: What You Need To KnowFavio Alvarez De BejarNoch keine Bewertungen
- 3 - NCM112Dokument6 Seiten3 - NCM112Edthel IniegoNoch keine Bewertungen
- Blunt Abdominal Trauma Watch and Wait.23Dokument8 SeitenBlunt Abdominal Trauma Watch and Wait.23carlosa.sierram98Noch keine Bewertungen
- GO ClindamycinDokument9 SeitenGO ClindamycinSAMANTHA T. MODESTONoch keine Bewertungen
- Journal Reading Neurovaskuler BanuDokument16 SeitenJournal Reading Neurovaskuler BanuBanu Eko SusantoNoch keine Bewertungen
- ACG Clinical Guideline Diagnosis and Management.17 PDFDokument21 SeitenACG Clinical Guideline Diagnosis and Management.17 PDFPrakashNoch keine Bewertungen
- G Epl PDFDokument39 SeitenG Epl PDFSaenab AminNoch keine Bewertungen
- NCCN Guideline RC v3 2022Dokument20 SeitenNCCN Guideline RC v3 2022dony hendrawanNoch keine Bewertungen
- 71) Cancer of The EsophagusDokument29 Seiten71) Cancer of The EsophagusANNA CarausNoch keine Bewertungen
- Operative Solutions in Hepatobiliary and Pancreatic SurgeryDokument352 SeitenOperative Solutions in Hepatobiliary and Pancreatic SurgerycirgeralNoch keine Bewertungen
- Diagnostic Laparoscopy in Penetrating Abdominal TraumaDokument4 SeitenDiagnostic Laparoscopy in Penetrating Abdominal TraumaNicolás Joel Peñalosa CupajitaNoch keine Bewertungen
- A Practical Review of Watch-And-WaitDokument8 SeitenA Practical Review of Watch-And-WaitAnitei GabrielaNoch keine Bewertungen
- If HP Cancer Guide Gu001 TesticularDokument23 SeitenIf HP Cancer Guide Gu001 TesticularwidyaputraNoch keine Bewertungen
- PREOPinguinalherniaDokument2 SeitenPREOPinguinalherniapatriciaatan1497Noch keine Bewertungen
- Barrett's Esophagus ACG 2017Dokument21 SeitenBarrett's Esophagus ACG 2017Adhytia PradiarthaNoch keine Bewertungen
- Screening Endometrial Web AlgorithmDokument3 SeitenScreening Endometrial Web AlgorithmKadir GümüşNoch keine Bewertungen
- Miscarriage or Early Pregnancy Loss-Diagnosis and ManagementDokument22 SeitenMiscarriage or Early Pregnancy Loss-Diagnosis and ManagementherryNoch keine Bewertungen
- Indeterminate Renal Mass ACR Appropriateness CriteriaDokument10 SeitenIndeterminate Renal Mass ACR Appropriateness CriteriaAndrew TaliaferroNoch keine Bewertungen
- Breast Specimen Handling and Reporting in The Postneoadjuvant Setting Challenges and AdvancesDokument13 SeitenBreast Specimen Handling and Reporting in The Postneoadjuvant Setting Challenges and AdvancesKarlaMaldonadoMonsalveNoch keine Bewertungen
- Jurnal Nilai Kritis LabDokument18 SeitenJurnal Nilai Kritis Labdesta jayantiNoch keine Bewertungen
- Righ Choise TrialDokument17 SeitenRigh Choise TrialOscar FloresNoch keine Bewertungen
- Neonatal Jaundice PathwayDokument35 SeitenNeonatal Jaundice Pathwaypragita ayu100% (1)
- Reproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesDokument28 SeitenReproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesFandoNoch keine Bewertungen
- A1 - Li, 2019Dokument8 SeitenA1 - Li, 2019bayu seno ajiNoch keine Bewertungen
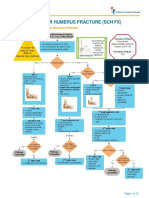
- Fracture Supracondylar HumerusDokument12 SeitenFracture Supracondylar HumeruskemsNoch keine Bewertungen
- PDFsam ObGynDokument4 SeitenPDFsam ObGynAlessandro ZadraNoch keine Bewertungen
- Contessa - Plante2019Dokument7 SeitenContessa - Plante2019moises vigilNoch keine Bewertungen
- Imaging Assessment of Hepatocellular Carcinoma Response To Locoregional and Systemic TherapyDokument19 SeitenImaging Assessment of Hepatocellular Carcinoma Response To Locoregional and Systemic Therapyanra kusumaNoch keine Bewertungen
- PearlsDokument2 SeitenPearlspatriciaatan1497Noch keine Bewertungen
- Complicaciones Endosco AltaDokument7 SeitenComplicaciones Endosco AltaJorge Adrian Romero SanchezNoch keine Bewertungen
- Surgical Management of Breast Cancer Treated With Neoadjuvant TherapyDokument6 SeitenSurgical Management of Breast Cancer Treated With Neoadjuvant TherapyIvory June CadeteNoch keine Bewertungen
- Diclofenac Drug StudyDokument1 SeiteDiclofenac Drug StudyMa. Sheenadel Zamudio100% (5)
- Atlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsVon EverandAtlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsFrieder BerrNoch keine Bewertungen
- Enfermedad de PagetDokument4 SeitenEnfermedad de PagetNicolás BertachiniNoch keine Bewertungen
- Cancer de Mama y EmbarazoDokument5 SeitenCancer de Mama y EmbarazoNicolás BertachiniNoch keine Bewertungen
- Committee Opinion No 624 Cervical Cancer.49Dokument3 SeitenCommittee Opinion No 624 Cervical Cancer.49Nicolás BertachiniNoch keine Bewertungen
- Committee Opinion No 588 Human Papillomavirus.42Dokument7 SeitenCommittee Opinion No 588 Human Papillomavirus.42Nicolás BertachiniNoch keine Bewertungen
- EndometriosisDokument5 SeitenEndometriosisNicolás BertachiniNoch keine Bewertungen
- Allen: BiologyDokument2 SeitenAllen: BiologySandeep JaiswalNoch keine Bewertungen
- (CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesDokument194 Seiten(CPG) Philippine Guidelines On Periodic Health Examination: Screening For Neoplastic DiseasesBianca Watanabe - RatillaNoch keine Bewertungen
- Nursing Dissertation CancerDokument6 SeitenNursing Dissertation CancerPaperWritingServiceReviewsSingapore100% (1)
- Answers To Common Questions About Breast Screening and MammogramsDokument5 SeitenAnswers To Common Questions About Breast Screening and MammogramsWatertown Daily TimesNoch keine Bewertungen
- 4909 PDFDokument2 Seiten4909 PDFMohamed MakkledNoch keine Bewertungen
- CV Jatin S GandhiDokument5 SeitenCV Jatin S GandhiSanjoy SanyalNoch keine Bewertungen
- BoneDokument35 SeitenBoneSumanth KaiwarNoch keine Bewertungen
- Idiopatik LeukoplakiaDokument2 SeitenIdiopatik LeukoplakiaAfiyatul IsnainiNoch keine Bewertungen
- Pathogenesis of Neoplasm PDFDokument3 SeitenPathogenesis of Neoplasm PDFTasya Citra KiranaNoch keine Bewertungen
- Cancer Colon and Rectum (Wardah)Dokument23 SeitenCancer Colon and Rectum (Wardah)WardahAliNoch keine Bewertungen
- Benign Odontogenic Tumors of Jaws (AmeloblastomaDokument70 SeitenBenign Odontogenic Tumors of Jaws (Ameloblastomagalina poberezhnikNoch keine Bewertungen
- Adjuvant ChemotheraphyDokument10 SeitenAdjuvant ChemotheraphyFatona AgungNoch keine Bewertungen
- Cervical CancerDokument27 SeitenCervical CancerHanif RezaNoch keine Bewertungen
- Plummer 2021Dokument6 SeitenPlummer 2021Cristina CostaNoch keine Bewertungen
- Anal CancerDokument36 SeitenAnal CancerBurhan MinervaNoch keine Bewertungen
- Why Black Women With Ovarian Cancer Require Greater FocusDokument1 SeiteWhy Black Women With Ovarian Cancer Require Greater FocusMicheleFontanaNoch keine Bewertungen
- Bilateral BreastDokument24 SeitenBilateral Breastamrul0776Noch keine Bewertungen
- ICRU Report 89-48-78Dokument31 SeitenICRU Report 89-48-78Sandra Johana Patino LeivaNoch keine Bewertungen
- Cervical Cancer Thesis StatementDokument6 SeitenCervical Cancer Thesis StatementBecky Goins100% (2)
- Chapter 21 - The Lower Urinary Tract and Male Genital SystemDokument38 SeitenChapter 21 - The Lower Urinary Tract and Male Genital SystemAgnieszka WisniewskaNoch keine Bewertungen
- Ginecomastia Ca Semn de Prezentare Intr-O Tumora TDokument5 SeitenGinecomastia Ca Semn de Prezentare Intr-O Tumora TClaudia IrimieNoch keine Bewertungen
- Article OralDokument36 SeitenArticle Oralamina-fakirproNoch keine Bewertungen
- Bowel StatisticsDokument2 SeitenBowel StatisticsbillpaparounisNoch keine Bewertungen
- Cholangiocarcinoma 2 Juni 2018Dokument40 SeitenCholangiocarcinoma 2 Juni 2018Anonymous 1UgsHkUNoch keine Bewertungen
- Concept MapDokument1 SeiteConcept MapSheryl Ann Barit PedinesNoch keine Bewertungen
- Pertemuan 10. Fitoterapi TumorDokument24 SeitenPertemuan 10. Fitoterapi TumorDila AprianiNoch keine Bewertungen
- GP 96Dokument24 SeitenGP 96Study MaterialNoch keine Bewertungen
- DECAL LNH Refrac JCO 2001Dokument7 SeitenDECAL LNH Refrac JCO 2001sunrasta23Noch keine Bewertungen