Das könnte Ihnen auch gefallen
- Supraclavicular Brachial Plexus BlockDokument2 SeitenSupraclavicular Brachial Plexus BlockmagedemanNoch keine Bewertungen
- Midface Fractures PART IIDokument64 SeitenMidface Fractures PART IIJomi Porinchu100% (1)
- Wound Healing: Dr. Shaimaa Alaraby Specialist of General SurgeryDokument21 SeitenWound Healing: Dr. Shaimaa Alaraby Specialist of General SurgeryOsama Fadel ahmedNoch keine Bewertungen
- Assignment: Shri Guru Ram Dass College of Nursing HoshiarpurDokument11 SeitenAssignment: Shri Guru Ram Dass College of Nursing HoshiarpurAman Chaudhary100% (2)
- Cesarean Section in Post-Polio PatientDokument2 SeitenCesarean Section in Post-Polio PatientasclepiuspdfsNoch keine Bewertungen
- Cervical Sympathectomy For Hyperhidrosis: A Report of Two CasesDokument6 SeitenCervical Sympathectomy For Hyperhidrosis: A Report of Two CasesTJPRC PublicationsNoch keine Bewertungen
- Hiperidrose, SCHICK, 2016Dokument7 SeitenHiperidrose, SCHICK, 2016Thalita HerekNoch keine Bewertungen
- Traumatic Diaphragmatic Hernia Anaesthetic ConsideDokument3 SeitenTraumatic Diaphragmatic Hernia Anaesthetic ConsideHalim SudonoNoch keine Bewertungen
- 1 PBDokument12 Seiten1 PBleomseveroNoch keine Bewertungen
- Endolymphatic Sac Surgery For Ménière 'S Disease - Current Opinion and Literature ReviewDokument5 SeitenEndolymphatic Sac Surgery For Ménière 'S Disease - Current Opinion and Literature Reviewknowledgeguruos179Noch keine Bewertungen
- Wound Management 2017Dokument9 SeitenWound Management 2017Carlos DNoch keine Bewertungen
- Thoracic Epidural For Modified Radical Mastectomy in A High-Risk PatientDokument2 SeitenThoracic Epidural For Modified Radical Mastectomy in A High-Risk PatientBianca CaterinalisendraNoch keine Bewertungen
- Laparoscopic Cholecystectomy Under Spinal Anaesthesia: A Prospective StudyDokument4 SeitenLaparoscopic Cholecystectomy Under Spinal Anaesthesia: A Prospective Studyrazaqhussain00Noch keine Bewertungen
- Obesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaDokument8 SeitenObesity and Anticipated Difficult Airway - A Comprehensive Approach With Videolaryngoscopy, Ramp Position, Sevoflurane and Opioid Free AnaesthesiaIJAR JOURNALNoch keine Bewertungen
- Bjorl: Surgical Treatment of Severe Laryngomalacia: A Retrospective Study of 11 CasesDokument5 SeitenBjorl: Surgical Treatment of Severe Laryngomalacia: A Retrospective Study of 11 CasesPutri HakimNoch keine Bewertungen
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Dokument4 SeitenComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNoch keine Bewertungen
- 2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRDokument2 Seiten2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRPoljarLijanNoch keine Bewertungen
- 5 Dexmedetomidine As Rescue Drug During Awake Craniotomy For Cortical Motor Mapping and Tumor Resection - Case Report - Anesth Analg 2006 1021556-8Dokument3 Seiten5 Dexmedetomidine As Rescue Drug During Awake Craniotomy For Cortical Motor Mapping and Tumor Resection - Case Report - Anesth Analg 2006 1021556-8Meenal Chauhan MendirattaNoch keine Bewertungen
- 9829 CE (Ra) F (SH) PF1 (SNAK) PFA (P)Dokument4 Seiten9829 CE (Ra) F (SH) PF1 (SNAK) PFA (P)razaqhussain00Noch keine Bewertungen
- Best Practice & Research Clinical Endocrinology & MetabolismDokument15 SeitenBest Practice & Research Clinical Endocrinology & MetabolismFernanda M. SoberonNoch keine Bewertungen
- JurnalDokument5 SeitenJurnalFuchsia ZeinNoch keine Bewertungen
- Anestesi Pada Fraktur MandibulaDokument11 SeitenAnestesi Pada Fraktur MandibulaCredo AriefNoch keine Bewertungen
- E Posters PDFDokument349 SeitenE Posters PDFpriyadikkalaNoch keine Bewertungen
- Neuromuscular Blockade Improves Surgical Conditions (NISCO)Dokument10 SeitenNeuromuscular Blockade Improves Surgical Conditions (NISCO)chrisi19781Noch keine Bewertungen
- Best Practice & Research Clinical Endocrinology & MetabolismDokument13 SeitenBest Practice & Research Clinical Endocrinology & MetabolismAhmad Harissul IbadNoch keine Bewertungen
- 40 The Manual Diaphragm Release Technique Improves Diaphragmatic MobilityDokument8 Seiten40 The Manual Diaphragm Release Technique Improves Diaphragmatic MobilityRenan O. Pravatta PivettaNoch keine Bewertungen
- Increased Lung Clearance of Isoflurane Shortens Emergence in Obesity: A Prospective Randomized-Controlled TrialDokument8 SeitenIncreased Lung Clearance of Isoflurane Shortens Emergence in Obesity: A Prospective Randomized-Controlled Trialale_rhdNoch keine Bewertungen
- Canmedaj01540 0049Dokument4 SeitenCanmedaj01540 0049ImanNoch keine Bewertungen
- Nej M 199905203402002Dokument6 SeitenNej M 199905203402002Ridwan Hadinata SalimNoch keine Bewertungen
- 2010 SimpatectomiaDokument8 Seiten2010 SimpatectomiaJavier VegaNoch keine Bewertungen
- H (HBOT) (AD) : Olish Yperbaric EsearchDokument6 SeitenH (HBOT) (AD) : Olish Yperbaric EsearchVera MHNoch keine Bewertungen
- Heiser2017 Article SelectiveUpperAirwayStimulatioDokument8 SeitenHeiser2017 Article SelectiveUpperAirwayStimulatioYondi Piter PapulungNoch keine Bewertungen
- Surgery 23 3 1Dokument6 SeitenSurgery 23 3 1razaqhussain00Noch keine Bewertungen
- Intrapleural CatheterDokument2 SeitenIntrapleural CatheterDr.Sandeep Kumar KarNoch keine Bewertungen
- US Pulmón para Manejo de Atelectasias PerioperatoriasDokument11 SeitenUS Pulmón para Manejo de Atelectasias PerioperatoriasJURAGOMANoch keine Bewertungen
- Erdem 2018Dokument9 SeitenErdem 2018SFS GAMEX546Noch keine Bewertungen
- Yjbm00011 0024Dokument6 SeitenYjbm00011 0024puskesmas perdanaNoch keine Bewertungen
- A Clinical Randomized Study On The Effects of Invasive Monitoring On Burn Shock ResuscitationDokument10 SeitenA Clinical Randomized Study On The Effects of Invasive Monitoring On Burn Shock ResuscitationHusni maiyantiNoch keine Bewertungen
- Anafilaxia MidazolamDokument3 SeitenAnafilaxia MidazolamDiana PintorNoch keine Bewertungen
- Mid Term Results of Pneumatic Balloon Dilatation in Patients With AchalasiaDokument3 SeitenMid Term Results of Pneumatic Balloon Dilatation in Patients With AchalasiaLuis PerazaNoch keine Bewertungen
- Mehu131 U2 T3 SindromeCushing3 PDFDokument14 SeitenMehu131 U2 T3 SindromeCushing3 PDFJoao Áandréeíí DíazNoch keine Bewertungen
- Guillen-Sola Et AlDokument7 SeitenGuillen-Sola Et AlLarisssaa FerreiraNoch keine Bewertungen
- Jove 87 50687aDokument15 SeitenJove 87 50687aSaúlNoch keine Bewertungen
- IcuDokument56 SeitenIcurulli_pranandaNoch keine Bewertungen
- 559 FullDokument5 Seiten559 FullSukhvinder Singh RanaNoch keine Bewertungen
- 7 Early Clinical Experience Using High Intensity Focused Ultrasound For Palliation of Inoperable Pancreatic CancerDokument7 Seiten7 Early Clinical Experience Using High Intensity Focused Ultrasound For Palliation of Inoperable Pancreatic CancerEvelynLisettVargasNoch keine Bewertungen
- OutDokument8 SeitenOutNosa Nosa SalossoNoch keine Bewertungen
- Haloperidol Combined With DexamethasoneDokument6 SeitenHaloperidol Combined With Dexamethasoneapi-741687858Noch keine Bewertungen
- Research ArticleDokument7 SeitenResearch Articlenaljnaby9Noch keine Bewertungen
- Background: Concurrent Chemoradiotherapy (CRT) Is The: Correspondence To: DR A.S.C. Wong, Department of HematologyDokument11 SeitenBackground: Concurrent Chemoradiotherapy (CRT) Is The: Correspondence To: DR A.S.C. Wong, Department of HematologyJordan SantosNoch keine Bewertungen
- The Use of Manual Hyperinflation in Airway Clearance: Series "Chest Physiotherapy" Edited by S.L. Hill and B. WebberDokument8 SeitenThe Use of Manual Hyperinflation in Airway Clearance: Series "Chest Physiotherapy" Edited by S.L. Hill and B. WebberHello RainbowNoch keine Bewertungen
- Srivastav A 2013Dokument4 SeitenSrivastav A 2013Putri YingNoch keine Bewertungen
- Research ArticleDokument7 SeitenResearch ArticleYosia KevinNoch keine Bewertungen
- Medical and Surgical ProcedureDokument13 SeitenMedical and Surgical Procedureprathamesh patilNoch keine Bewertungen
- 2015 Article 327Dokument6 Seiten2015 Article 327Rafael FontesNoch keine Bewertungen
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDokument9 SeitenEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNoch keine Bewertungen
- E423 FullDokument11 SeitenE423 FullCecepNoch keine Bewertungen
- Amila HanifaDokument10 SeitenAmila HanifaDanang Budi SetiawanNoch keine Bewertungen
- tmp9204 TMPDokument4 Seitentmp9204 TMPFrontiersNoch keine Bewertungen
- Photodynamic Therapy (PDT) For Lung Cancer: The Yorkshire Laser Centre ExperienceDokument10 SeitenPhotodynamic Therapy (PDT) For Lung Cancer: The Yorkshire Laser Centre ExperienceRahmahh FyyNoch keine Bewertungen
- Ropvacaina VS Lidocaina Premdicacion IotDokument6 SeitenRopvacaina VS Lidocaina Premdicacion IotFaith Lu PenalozaNoch keine Bewertungen
- Anesthesia in Thoracic Surgery: Changes of ParadigmsVon EverandAnesthesia in Thoracic Surgery: Changes of ParadigmsManuel Granell GilNoch keine Bewertungen
- Kode Tindakan OperasiDokument5 SeitenKode Tindakan Operasijoko ismulyanto100% (1)
- Avelar Abdoplasty ExpDokument5 SeitenAvelar Abdoplasty Exprandomaeiou7273Noch keine Bewertungen
- Announcement Fiesta Urologi 2017Dokument8 SeitenAnnouncement Fiesta Urologi 2017Alfin KamalNoch keine Bewertungen
- Aesculap CaimanDokument6 SeitenAesculap CaimanAnonymous Qo6L9YQsdNoch keine Bewertungen
- Ahead,: Is What We AreDokument10 SeitenAhead,: Is What We AreKothapalli ChiranjeeviNoch keine Bewertungen
- Supine PCNL in Patient With Staghorn Renal Stone ADokument4 SeitenSupine PCNL in Patient With Staghorn Renal Stone AhasanyahyadrNoch keine Bewertungen
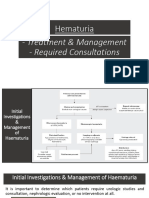
- Hematuria Treatment Management and Required ConsultationsDokument10 SeitenHematuria Treatment Management and Required ConsultationsDiyana ZatyNoch keine Bewertungen
- Otolaryngology - Head and Neck Surgery: Fracture Patterns of The Nasal SeptumDokument6 SeitenOtolaryngology - Head and Neck Surgery: Fracture Patterns of The Nasal SeptumEduardo Cantu GarzaNoch keine Bewertungen
- Michigan Manual of Plastic Surgery: Aesthetic Surgery Journal April 2015Dokument3 SeitenMichigan Manual of Plastic Surgery: Aesthetic Surgery Journal April 2015Mayerlin CalvacheNoch keine Bewertungen
- Daftar PustakaDokument6 SeitenDaftar Pustakarifa salsabilahNoch keine Bewertungen
- Daftar Pustaka Refrat Bedah PlastikDokument3 SeitenDaftar Pustaka Refrat Bedah PlastikAnggita DewiNoch keine Bewertungen
- Urinary Tract InfectionDokument2 SeitenUrinary Tract InfectionSANDYTHYANoch keine Bewertungen
- 1.introduction To Sports InjuriesDokument17 Seiten1.introduction To Sports InjuriesKhurram ShahzadNoch keine Bewertungen
- RGU and MCU PPT Final For 18.9.23, BsmmuDokument46 SeitenRGU and MCU PPT Final For 18.9.23, BsmmuMd.AlauddinNoch keine Bewertungen
- DR - KumarSonal No CVDokument3 SeitenDR - KumarSonal No CVashish bondiaNoch keine Bewertungen
- 6 Ab 2Dokument3 Seiten6 Ab 2Erko100% (1)
- A Novel Technique For Exeter Stem Extraction.8Dokument2 SeitenA Novel Technique For Exeter Stem Extraction.8Mohan DesaiNoch keine Bewertungen
- ! CASE REPORT Athaya FIXED Kumpul SekreDokument23 Seiten! CASE REPORT Athaya FIXED Kumpul SekreFusarina MumpuniNoch keine Bewertungen
- 4.3.3 - Part I 3Dokument2 Seiten4.3.3 - Part I 3Victoria FuenmayorNoch keine Bewertungen
- Colporrhaphy: Rajah Amina SuleimanDokument20 SeitenColporrhaphy: Rajah Amina SuleimanAmina RajahNoch keine Bewertungen
- Return Invoice 231.8.2023Dokument2 SeitenReturn Invoice 231.8.2023ahmed.zulkhaireNoch keine Bewertungen
- Captain America's Shield GenioplastyDokument3 SeitenCaptain America's Shield GenioplastyVarun bharathi100% (1)
- EAU Pocket On Non Neurogenic Male LUTS 2022Dokument26 SeitenEAU Pocket On Non Neurogenic Male LUTS 2022AlbalushiNoch keine Bewertungen
- Jadwal Dokter TerbaruDokument1 SeiteJadwal Dokter Terbaruphn kitchen idNoch keine Bewertungen
- Rajasthan Government Health Scheme: List of Empaneled Hospitals As On 08-03-2022Dokument8 SeitenRajasthan Government Health Scheme: List of Empaneled Hospitals As On 08-03-2022Ravindra RathoreNoch keine Bewertungen
- 539-Article Text-3893-3-10-20201103Dokument9 Seiten539-Article Text-3893-3-10-20201103Indah MadaNoch keine Bewertungen
- Altrazeal® Application Guide 2.0 VFDokument2 SeitenAltrazeal® Application Guide 2.0 VFdeeepNoch keine Bewertungen
- SINGI Solved Papers of ENTDokument430 SeitenSINGI Solved Papers of ENTjbtcmdtjjvNoch keine Bewertungen