Das könnte Ihnen auch gefallen
- Rules and Directions for the Employment of Injections in Various DiseasesVon EverandRules and Directions for the Employment of Injections in Various DiseasesNoch keine Bewertungen
- Alteration of The Starling Forces Which Control Transfer of Fluid From The Vascular Compartment To Surrounding Tissue SpacesDokument3 SeitenAlteration of The Starling Forces Which Control Transfer of Fluid From The Vascular Compartment To Surrounding Tissue SpacesNicole cuencosNoch keine Bewertungen
- Post-cholecystectomy Bile Duct InjuryVon EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNoch keine Bewertungen
- NCP BPHDokument8 SeitenNCP BPHjyaba0% (1)
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesVon EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesBewertung: 5 von 5 Sternen5/5 (2)
- Nursing Care PlansDokument4 SeitenNursing Care Planswerismy daddyNoch keine Bewertungen
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesVon EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesNoch keine Bewertungen
- CuesDokument2 SeitenCuesFrance SuarezNoch keine Bewertungen
- A Man’s Guide to Bladder Problems & Urinary IncontinenceVon EverandA Man’s Guide to Bladder Problems & Urinary IncontinenceNoch keine Bewertungen
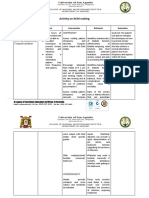
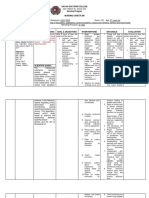
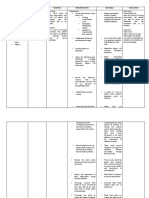
- Activity On NCM MakingDokument4 SeitenActivity On NCM MakingJollan Marie BuenvenidaNoch keine Bewertungen
- Bladder Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandBladder Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- NURSING CARE PLAN - Impaired Urinary EliminationDokument2 SeitenNURSING CARE PLAN - Impaired Urinary EliminationDaniel Andre S. SomorayNoch keine Bewertungen
- Interpretation of Urodynamic Studies: A Case Study-Based GuideVon EverandInterpretation of Urodynamic Studies: A Case Study-Based GuideNoch keine Bewertungen
- Nursing Care PlansDokument4 SeitenNursing Care PlansanreilegardeNoch keine Bewertungen
- Diverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookVon EverandDiverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookNoch keine Bewertungen
- Benign Prostatic Hyperplasia. NCM 109Dokument16 SeitenBenign Prostatic Hyperplasia. NCM 109Niña Jean Tormis AldabaNoch keine Bewertungen
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesVon EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesBewertung: 1 von 5 Sternen1/5 (1)
- Impaired Urinary EliminationDokument2 SeitenImpaired Urinary EliminationSiafei RabeNoch keine Bewertungen
- A Simple Guide To Nocturia, (Excessive Night Urination) Diagnosis, Treatment And Related ConditionsVon EverandA Simple Guide To Nocturia, (Excessive Night Urination) Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Assignment in NCM 106 LectureDokument6 SeitenAssignment in NCM 106 LectureJeanessa Delantar QuilisadioNoch keine Bewertungen
- Nursing Care in MR.X With Urinary Retention: Disusun OlehDokument4 SeitenNursing Care in MR.X With Urinary Retention: Disusun OlehHafin WardanaNoch keine Bewertungen
- NCP - Mod9Dokument3 SeitenNCP - Mod9designericlelynsoronioNoch keine Bewertungen
- NCPDokument2 SeitenNCPbulok netflakesNoch keine Bewertungen
- NCP - Impaired Urinary EliminationDokument3 SeitenNCP - Impaired Urinary EliminationFretzgine Lou ManuelNoch keine Bewertungen
- Gonzales - Nursing Care Plan - Intrapartal CareDokument3 SeitenGonzales - Nursing Care Plan - Intrapartal CareTrixiaNoch keine Bewertungen
- Nursing Care Plan On CystoceleDokument7 SeitenNursing Care Plan On Cystoceleleo100% (1)
- Nursing Care PlanDokument2 SeitenNursing Care Planmjoie_baby6568470100% (6)
- NCP - Impaire Urinary EliminationDokument3 SeitenNCP - Impaire Urinary EliminationNicole cuencosNoch keine Bewertungen
- Risk For Fluid VolumeDokument1 SeiteRisk For Fluid VolumeMariella BadongenNoch keine Bewertungen
- NCP Urinary RetentionDokument3 SeitenNCP Urinary RetentionKingJayson Pacman06Noch keine Bewertungen
- Nursing Care Plan: Assessment Diagnosis Goals Intervention Rationale EvaluationDokument2 SeitenNursing Care Plan: Assessment Diagnosis Goals Intervention Rationale EvaluationLeizel ApolonioNoch keine Bewertungen
- Davao Doctors College Nursing Program Nursing Care PlanDokument3 SeitenDavao Doctors College Nursing Program Nursing Care PlanPRINCESS KOBAYASHINoch keine Bewertungen
- DS - Senokot ForteDokument1 SeiteDS - Senokot ForteMarjorie Dela RosaNoch keine Bewertungen
- NCP Urine RetentionDokument4 SeitenNCP Urine RetentionKingJayson Pacman06Noch keine Bewertungen
- NCP (BPH)Dokument8 SeitenNCP (BPH)NataCo50% (2)
- La Salle University Nursing Care PlanDokument3 SeitenLa Salle University Nursing Care PlanJb RosillosaNoch keine Bewertungen
- NCP BPHDokument1 SeiteNCP BPHyasiraNoch keine Bewertungen
- Impaired Urinary EliminationDokument3 SeitenImpaired Urinary EliminationDenise Republika100% (1)
- NCP Impaired Urinary EliminationDokument2 SeitenNCP Impaired Urinary EliminationTrixy Marie EcotNoch keine Bewertungen
- Borata Nursing Process RleDokument11 SeitenBorata Nursing Process Rlefiel borataNoch keine Bewertungen
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetDokument3 SeitenAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetPrincess Mildred AbdonNoch keine Bewertungen
- Silvaqueenie Rose Multiple SclerosisDokument5 SeitenSilvaqueenie Rose Multiple SclerosisQueenie SilvaNoch keine Bewertungen
- Nursing Care Plan (NCP) For A Patient With Acute Renal FailureDokument3 SeitenNursing Care Plan (NCP) For A Patient With Acute Renal FailureKian HerreraNoch keine Bewertungen
- NCP-Acute Gastroenteritis PediatricDokument11 SeitenNCP-Acute Gastroenteritis PediatricJhoevina Dulce Capicio0% (1)
- Deficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientDokument2 SeitenDeficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientSeanmarie CabralesNoch keine Bewertungen
- Nursing Care Plan Impaired Urinary EliminationDokument1 SeiteNursing Care Plan Impaired Urinary Eliminationderic86% (14)
- Group-5 NCM-107 NCPDokument4 SeitenGroup-5 NCM-107 NCPbulok netflakes100% (1)
- NCP For Acute Gastroenteritis (Pediatric)Dokument6 SeitenNCP For Acute Gastroenteritis (Pediatric)abcel76% (21)
- NCP FinalDokument6 SeitenNCP FinalWanwan PraybeytNoch keine Bewertungen
- Assessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleDokument4 SeitenAssessment Diagnosis Planning Interventions Evaluation Nsg. Action RationaleRhea Mae Valles - ReyesNoch keine Bewertungen
- Diarrhea Nursing Care PlanDokument2 SeitenDiarrhea Nursing Care PlanKrizha Angela NicolasNoch keine Bewertungen
- Aquino NCP UtiDokument3 SeitenAquino NCP UtiGianne ObaldoNoch keine Bewertungen
- Urinary Bladder MassDokument2 SeitenUrinary Bladder Masskarl de guzmanNoch keine Bewertungen
- Excess Fluid Volume Related To Sodium IntakeDokument5 SeitenExcess Fluid Volume Related To Sodium IntakeNil GyiNoch keine Bewertungen
- Subjective: Long Term Objective: Long Term ObjectiveDokument2 SeitenSubjective: Long Term Objective: Long Term ObjectiveRAFNoch keine Bewertungen
- NCP Deficient Fluid VolumeDokument3 SeitenNCP Deficient Fluid VolumeDoneva Lyn MedinaNoch keine Bewertungen
- Nursing-Care-Plan - AgeDokument7 SeitenNursing-Care-Plan - AgePanda JocyNoch keine Bewertungen
- NCP Pedia RotDokument5 SeitenNCP Pedia RotGian kyle AradillosNoch keine Bewertungen
- Subjective: The Client's Grandmother Stated " Hindi Pa Nga Siya Dumudumi Simula Nung Nahospital Siya Ngayon. Mga Apat Na Araw Na Ata." ObjectiveDokument2 SeitenSubjective: The Client's Grandmother Stated " Hindi Pa Nga Siya Dumudumi Simula Nung Nahospital Siya Ngayon. Mga Apat Na Araw Na Ata." ObjectiveAngelou MortosNoch keine Bewertungen
- 15 UrinalysisDokument9 Seiten15 UrinalysisJaney Ceniza تNoch keine Bewertungen
- CV 2023010319584829Dokument1 SeiteCV 2023010319584829Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- Pnle ReviewerDokument293 SeitenPnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- Daniel Saladas ResumeDokument2 SeitenDaniel Saladas ResumeAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Application Forms (Fillable)Dokument2 SeitenApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- Nursing Notes Maternal and Child Nursing CareDokument70 SeitenNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- DSWDDokument3 SeitenDSWDAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Credential Verification Form Non-Clinical (Without Signature Page)Dokument1 SeiteCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- To Fill-Up Id-Atm FormDokument7 SeitenTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- FNCP PoorsanitationmarwahDokument3 SeitenFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- LargoDokument1 SeiteLargoAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- KNOWLEGDEDEFICITFNCPDokument2 SeitenKNOWLEGDEDEFICITFNCPAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Introduction IntroDokument2 SeitenIntroduction IntroAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Introduction IntroDokument2 SeitenIntroduction IntroAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Health Teaching Plan FinaleDokument4 SeitenHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Poor Environmetal Sanitation As Health Threat CuesDokument11 SeitenPoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case StudyDokument33 SeitenFamily Case StudyAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case Study PresentationDokument1 SeiteFamily Case Study PresentationAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- LargoDokument1 SeiteLargoAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Poor Compliance With Treatment As Health Threat CuesDokument11 SeitenPoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case StudyDokument33 SeitenFamily Case StudyAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- NCPDokument2 SeitenNCPAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Gaid - IntroductionDokument5 SeitenGaid - IntroductionAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case Study On Pulmonary TuberculosisDokument4 SeitenFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- MocaaaaaDokument59 SeitenMocaaaaaAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDokument6 SeitenOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- FNCPDokument1 SeiteFNCPAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Mock ResumeDokument3 SeitenMock ResumeAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- 1 DrugsDokument2 Seiten1 DrugsPatricia Lucero100% (2)
- Introduction HiDokument4 SeitenIntroduction HiAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Health EDUC Teaching Demo RubricsDokument4 SeitenHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
- Ayurvedagram Case StudyDokument46 SeitenAyurvedagram Case StudyDarshan Bharde100% (4)
- ISONIAZIDDokument2 SeitenISONIAZIDXerxes DejitoNoch keine Bewertungen
- Pneumonia QuizDokument7 SeitenPneumonia QuizJennah JozelleNoch keine Bewertungen
- Clinical Uses of Diode Lasers in Orthodontics PDFDokument8 SeitenClinical Uses of Diode Lasers in Orthodontics PDFmonwarul azizNoch keine Bewertungen
- Squash Seeds FinalDokument19 SeitenSquash Seeds FinalMae TomeldenNoch keine Bewertungen
- Dentosphere - World of Dentistry - MCQs On Skin and Vesiculobullous Diseases - Or-SearchableDokument22 SeitenDentosphere - World of Dentistry - MCQs On Skin and Vesiculobullous Diseases - Or-SearchableAssssssNoch keine Bewertungen
- First Aid Booklet: Transition Passport / Daily Living / HealthDokument11 SeitenFirst Aid Booklet: Transition Passport / Daily Living / Healthmaggie HurleyNoch keine Bewertungen
- Seminar ON Seizure: Presented To Presented byDokument35 SeitenSeminar ON Seizure: Presented To Presented byShitaljit IromNoch keine Bewertungen
- Badminton Benefits and Disadvantages 431 Mvfik0Dokument2 SeitenBadminton Benefits and Disadvantages 431 Mvfik0SharathRaj0% (1)
- Unit 7 - Digestive System Guided Notes - VaughanDokument9 SeitenUnit 7 - Digestive System Guided Notes - VaughanJeanette IrambonaNoch keine Bewertungen
- Nomenklatur IBS Edit THTDokument291 SeitenNomenklatur IBS Edit THTriezki_pattikratonMDNoch keine Bewertungen
- A Framework For Mental Health ResearchDokument53 SeitenA Framework For Mental Health ResearchCriticalEyeNoch keine Bewertungen
- Clinical Assessment of A Psychiatric PatientDokument5 SeitenClinical Assessment of A Psychiatric PatientAlex AthanNoch keine Bewertungen
- Vii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowDokument2 SeitenVii. Laboratory Results: Hemoglobin 129 MG/DL 140-160 MG/DL LowAdrian Dela CruzNoch keine Bewertungen
- The Red Book ELSO 5th EditionDokument868 SeitenThe Red Book ELSO 5th EditionMohsinPasha67% (3)
- If Claim Rejected Due To Justification Not SatisfiedDokument10 SeitenIf Claim Rejected Due To Justification Not Satisfiedshivam.kumar1Noch keine Bewertungen
- What Is Tinnitus 911?: Vitamin BDokument4 SeitenWhat Is Tinnitus 911?: Vitamin Bشکیب لطیفNoch keine Bewertungen
- DR Enechukwu - Cutaneous Manifestations in Internal MalignancyDokument43 SeitenDR Enechukwu - Cutaneous Manifestations in Internal MalignancyMillicent AwuzieNoch keine Bewertungen
- 9.cancer of The Female Genital Tract.Dokument58 Seiten9.cancer of The Female Genital Tract.vichramNoch keine Bewertungen
- Rguhs Thesis Topics in Oral MedicineDokument7 SeitenRguhs Thesis Topics in Oral Medicinemeganmoorearlington100% (2)
- Health Quarter 3 - Module 1 Health Trends, Issues and Concerns (Global Level)Dokument56 SeitenHealth Quarter 3 - Module 1 Health Trends, Issues and Concerns (Global Level)Janice Cajepe67% (3)
- Case CA StomachDokument23 SeitenCase CA StomachBrutus AntonyNoch keine Bewertungen
- Internet of Nano, Bio-Nano, Biodegradable And-3-4Dokument2 SeitenInternet of Nano, Bio-Nano, Biodegradable And-3-47d96d1b6a8Noch keine Bewertungen
- Hypovolemic Shock PathophysiologyDokument8 SeitenHypovolemic Shock PathophysiologyKAYCEENoch keine Bewertungen
- EKG Quick and Dirty - GD v3.0Dokument2 SeitenEKG Quick and Dirty - GD v3.0Sheema Sh100% (1)
- Dengue ICT NS1 PDFDokument7 SeitenDengue ICT NS1 PDFAsti Rizki Arum PermanaNoch keine Bewertungen
- Aquaculture Set IDokument17 SeitenAquaculture Set IClinton VillaflorNoch keine Bewertungen
- Community Based Assessment Checklist (CBAC) FormDokument3 SeitenCommunity Based Assessment Checklist (CBAC) FormShubhaDavalgiNoch keine Bewertungen
- Molecules of Life PDFDokument113 SeitenMolecules of Life PDFArpit Pradhan100% (1)
- Đề Giữa Kì 1 Anh 9 Tđ 21-22Dokument3 SeitenĐề Giữa Kì 1 Anh 9 Tđ 21-22Hoàng Ngân NguyễnNoch keine Bewertungen