Das könnte Ihnen auch gefallen
- Breaking the Chains: Understanding Substance Use Disorders and Mental HealthVon EverandBreaking the Chains: Understanding Substance Use Disorders and Mental HealthNoch keine Bewertungen
- Nu 12113564Dokument24 SeitenNu 12113564Laura CanoNoch keine Bewertungen
- Substance Abuse Group Therapy Activities for Adults: A Comprehensive Guide to Group Activities and Techniques for Overcoming Addiction: Group Therapy Activities For Addiction RecoveryVon EverandSubstance Abuse Group Therapy Activities for Adults: A Comprehensive Guide to Group Activities and Techniques for Overcoming Addiction: Group Therapy Activities For Addiction RecoveryNoch keine Bewertungen
- The Main Causes of Drug Abuse in The CommunityDokument3 SeitenThe Main Causes of Drug Abuse in The Communitygenelord opallaNoch keine Bewertungen
- Autonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaVon EverandAutonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaNoch keine Bewertungen
- 1 s2.0 S0028390821001106 MainDokument29 Seiten1 s2.0 S0028390821001106 MainElisa RodríguezNoch keine Bewertungen
- Drugs and Substance AbuseDokument4 SeitenDrugs and Substance Abusevaibhavch2904Noch keine Bewertungen
- Drug Addiction TreatmentDokument47 SeitenDrug Addiction Treatmenthofmann.felipeNoch keine Bewertungen
- Drugs Apy 205Dokument22 SeitenDrugs Apy 205LiviaNoch keine Bewertungen
- Yau, Stress Eating Behaviors, 2013Dokument17 SeitenYau, Stress Eating Behaviors, 2013Maribel Ruiz BurgaNoch keine Bewertungen
- Principles of Drug Addiction Treatment A Research Based Guide Third EditionDokument67 SeitenPrinciples of Drug Addiction Treatment A Research Based Guide Third EditionКонстантин Крахмалев100% (1)
- Title - Understanding Drug Abuse - A Physiological Perspective-1Dokument7 SeitenTitle - Understanding Drug Abuse - A Physiological Perspective-1zeeshanhaiderm007Noch keine Bewertungen
- Drug AbuseDokument2 SeitenDrug Abusetafolabi473Noch keine Bewertungen
- 01616-Report 2003-01-31 1Dokument48 Seiten01616-Report 2003-01-31 1losangelesNoch keine Bewertungen
- The Science of AddictionDokument32 SeitenThe Science of AddictionKayciNoch keine Bewertungen
- Bipolar EditedDokument10 SeitenBipolar EditedRachael KaburuNoch keine Bewertungen
- Addiction Is A Brain DiseaseDokument4 SeitenAddiction Is A Brain Diseasehpdude3Noch keine Bewertungen
- Tratamiento Cognitivo para AdiccionesDokument12 SeitenTratamiento Cognitivo para AdiccionesJuanyfeny Carmilema FajardoNoch keine Bewertungen
- Food Reward SystemDokument12 SeitenFood Reward SystemCamilla MendesNoch keine Bewertungen
- Review of Related LiteratureDokument2 SeitenReview of Related LiteratureWinston PlarizaNoch keine Bewertungen
- 675 Principles of Drug Addiction Treatment A Research Based Guide Third EditionDokument75 Seiten675 Principles of Drug Addiction Treatment A Research Based Guide Third EditionVivek VatsNoch keine Bewertungen
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDokument26 SeitenRajiv Gandhi University of Health Sciences, Bangalore, KarnatakaAmit TamboliNoch keine Bewertungen
- Polypharmacy, Interactions and Collaborative Care in The Middle-Aged and Beyond. LB Stargrove and MB Stargrove (2012)Dokument8 SeitenPolypharmacy, Interactions and Collaborative Care in The Middle-Aged and Beyond. LB Stargrove and MB Stargrove (2012)adsfadfsfadafdNoch keine Bewertungen
- Drugfacts Understanding DrugDokument5 SeitenDrugfacts Understanding DrugGabriel David LievanoNoch keine Bewertungen
- Addictive BehavioursDokument4 SeitenAddictive BehavioursJoe HEATHNoch keine Bewertungen
- Ijerph 18 11269Dokument9 SeitenIjerph 18 11269driveamadeaNoch keine Bewertungen
- Soa PDFDokument32 SeitenSoa PDFJohnNoch keine Bewertungen
- Substance Abuse RecoveryDokument18 SeitenSubstance Abuse RecoveryDan BecarNoch keine Bewertungen
- Статья "Understanding Drug Use and Addiction" от National Institute on Drug AbuseDokument5 SeitenСтатья "Understanding Drug Use and Addiction" от National Institute on Drug AbuseGean LonskayaNoch keine Bewertungen
- Order 5206105Dokument9 SeitenOrder 5206105augustus muliNoch keine Bewertungen
- Ejemplo Ultra-Processed Food Consumption and Mental Health - A Systematic Review and Meta-Analysis of Observational StudiesDokument22 SeitenEjemplo Ultra-Processed Food Consumption and Mental Health - A Systematic Review and Meta-Analysis of Observational StudiesDiana PSNoch keine Bewertungen
- Term PaperDokument4 SeitenTerm PaperIvin KuriakoseNoch keine Bewertungen
- Contributions of Behavioral Science in Medicine: Palestine Polytechnic UniversityDokument4 SeitenContributions of Behavioral Science in Medicine: Palestine Polytechnic UniversityYazeed AsrawiNoch keine Bewertungen
- Impact of Wholeofdiet Interventions On Depression and Anxiety A Systematic Review of Randomised Controlled TrialsDokument20 SeitenImpact of Wholeofdiet Interventions On Depression and Anxiety A Systematic Review of Randomised Controlled Trialsgiulia.santinNoch keine Bewertungen
- Fall 2022 CultivateDokument15 SeitenFall 2022 CultivateFlorida Horticulture for Health NetworkNoch keine Bewertungen
- Drug Abuse in Society (Auto Recovered)Dokument27 SeitenDrug Abuse in Society (Auto Recovered)vanshika.bajakNoch keine Bewertungen
- Functional Health Patterns GordonDokument18 SeitenFunctional Health Patterns GordonJen BallesterosNoch keine Bewertungen
- G122088 Rizky Hadiansah ReportDokument2 SeitenG122088 Rizky Hadiansah ReportRizky HadiansahNoch keine Bewertungen
- Contributions of Behavioral Science in Medicine: Palestine Polytechnic UniversityDokument4 SeitenContributions of Behavioral Science in Medicine: Palestine Polytechnic UniversityYazeed AsrawiNoch keine Bewertungen
- Drugs, The Science of Addiction D Rugs, Brains, and BehaviorDokument36 SeitenDrugs, The Science of Addiction D Rugs, Brains, and Behavioritalianurses100% (1)
- Readings in Human BehaviorDokument4 SeitenReadings in Human BehaviorKael AsonyabNoch keine Bewertungen
- Nutritional Status and Eating Habits of People Who Use Drugs And:or Are Undergoing Treatment For RecoveryDokument9 SeitenNutritional Status and Eating Habits of People Who Use Drugs And:or Are Undergoing Treatment For RecoveryDevvi WidyaningrumNoch keine Bewertungen
- Ijerph 18 09791Dokument10 SeitenIjerph 18 09791Elisa RodríguezNoch keine Bewertungen
- Chapter 2 NeurobiologyDokument31 SeitenChapter 2 Neurobiologyanitha1118Noch keine Bewertungen
- What Is Functional MedicineDokument2 SeitenWhat Is Functional MedicineimanfekryahmedNoch keine Bewertungen
- Medical Interventions - EditedDokument4 SeitenMedical Interventions - EditedSharonNoch keine Bewertungen
- Drug AbuseDokument3 SeitenDrug Abusebelicariojamaica75Noch keine Bewertungen
- Mindfulness-Based Interventions For Obesity-Related Eating Behaviors: A Literature ReviewDokument20 SeitenMindfulness-Based Interventions For Obesity-Related Eating Behaviors: A Literature ReviewEliseia CarvalhoNoch keine Bewertungen
- Principles of Drug Abuse Treatment For: Criminal Justice PopulationsDokument18 SeitenPrinciples of Drug Abuse Treatment For: Criminal Justice PopulationslosangelesNoch keine Bewertungen
- Genes and AddictionsDokument7 SeitenGenes and AddictionsMihaela DumitrescuNoch keine Bewertungen
- Drug FactsDokument2 SeitenDrug FactsSiria PinedaNoch keine Bewertungen
- Nutrients 15 03715Dokument26 SeitenNutrients 15 03715TadijaNoch keine Bewertungen
- Transition PaperDokument9 SeitenTransition PaperAnonymous utfuIcnNoch keine Bewertungen
- NUTRIONDokument11 SeitenNUTRIONZuhaib AhmedNoch keine Bewertungen
- The Caused and Risk of Drugs On AdolescentsDokument20 SeitenThe Caused and Risk of Drugs On AdolescentsSyra Mae LausaNoch keine Bewertungen
- Drug and Alcohol Dependence: ReviewDokument11 SeitenDrug and Alcohol Dependence: ReviewCharlotte KeckhutNoch keine Bewertungen
- Risks of Self-Medication PracticesDokument28 SeitenRisks of Self-Medication PracticesFaizaNadeemNoch keine Bewertungen
- Aplicación Universidad de AarhusDokument21 SeitenAplicación Universidad de AarhusFrancisca Cabezas HenríquezNoch keine Bewertungen
- Geriatrics Gerontology Int - 2023 - KuzuyaDokument13 SeitenGeriatrics Gerontology Int - 2023 - Kuzuyamadiha ayubNoch keine Bewertungen
- NationalDokument14 SeitenNationallosangelesNoch keine Bewertungen
- Dose of Jogging and Long-Term Mortality: The Copenhagen City Heart StudyDokument9 SeitenDose of Jogging and Long-Term Mortality: The Copenhagen City Heart StudyCharles SeekNoch keine Bewertungen
- Free Printable Daily Excel PlannerDokument2 SeitenFree Printable Daily Excel PlannerCharles SeekNoch keine Bewertungen
- WADA Monitoring Program 2014 enDokument1 SeiteWADA Monitoring Program 2014 enCharles SeekNoch keine Bewertungen
- Up Your Bench Press 30lbs in 30 DaysDokument24 SeitenUp Your Bench Press 30lbs in 30 DaysCharles SeekNoch keine Bewertungen
- Starlift MetricDokument2 SeitenStarlift MetricCralesNoch keine Bewertungen
- Favino Circulation of Scientific Knowledge AcroDokument8 SeitenFavino Circulation of Scientific Knowledge AcroPeter FryNoch keine Bewertungen
- Bioclim MaxentDokument9 SeitenBioclim MaxentNicolás FrutosNoch keine Bewertungen
- Disorders of The Endocrine System and Dental ManagementDokument63 SeitenDisorders of The Endocrine System and Dental ManagementSanni FatimaNoch keine Bewertungen
- Shri Fa 4Dokument44 SeitenShri Fa 4Veena H NayakNoch keine Bewertungen
- 447.010 Screen Operating Manual v001Dokument67 Seiten447.010 Screen Operating Manual v001José CarlosNoch keine Bewertungen
- CF1900SS-DF Example Spec - Rev1Dokument1 SeiteCF1900SS-DF Example Spec - Rev1parsiti unnesNoch keine Bewertungen
- A Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFDokument2 SeitenA Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFPutra GagahNoch keine Bewertungen
- DalmatiaDokument265 SeitenDalmatiaomissam2Noch keine Bewertungen
- DHI-ITALE-060AA-P: White Strobe LampDokument2 SeitenDHI-ITALE-060AA-P: White Strobe LampXlabs MedanNoch keine Bewertungen
- Maxon - Gas Electro-Mechanical ValvesDokument4 SeitenMaxon - Gas Electro-Mechanical ValvesThiagoNoch keine Bewertungen
- Elevator ControlDokument3 SeitenElevator ControlNATHANNoch keine Bewertungen
- Glass Standards PDFDokument4 SeitenGlass Standards PDFCristian TofanNoch keine Bewertungen
- ISNGI 2017 ProgrammeDokument6 SeitenISNGI 2017 ProgrammeJoanna JohnsonNoch keine Bewertungen
- NEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andDokument90 SeitenNEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andliyanderNoch keine Bewertungen
- Prince Hydraulics Wolverine Adjustable Flow Control Valve Offered by PRC Industrial SupplyDokument1 SeitePrince Hydraulics Wolverine Adjustable Flow Control Valve Offered by PRC Industrial SupplyPRC Industrial SupplyNoch keine Bewertungen
- The Effective SpanDokument4 SeitenThe Effective SpanMohamed FarahNoch keine Bewertungen
- Dell Inspiron 16 5000 (5625) Laptop - Dell IndiaDokument5 SeitenDell Inspiron 16 5000 (5625) Laptop - Dell IndiamubbunNoch keine Bewertungen
- 120Dokument349 Seiten120xdyj2005Noch keine Bewertungen
- 100 Câu Viết Lại Câu Ôn Thi Vào Lóp 6Dokument10 Seiten100 Câu Viết Lại Câu Ôn Thi Vào Lóp 6Nguyễn Thanh PhươngNoch keine Bewertungen
- Electromagnetic and Thermal AnalysisDokument5 SeitenElectromagnetic and Thermal AnalysishamidrezaNoch keine Bewertungen
- Morality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordDokument3 SeitenMorality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordTHEO DOMINIC REQUERME SILVOSANoch keine Bewertungen
- Heil 4000 FeaturesDokument1 SeiteHeil 4000 FeaturesBogdan NgrNoch keine Bewertungen
- Fighting The Sixth Mass ExtinctionDokument25 SeitenFighting The Sixth Mass ExtinctionRichard J. MarksNoch keine Bewertungen
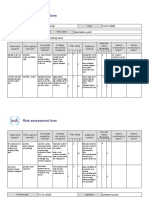
- Risk Assessment Project Iosh - MsDokument2 SeitenRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- XL4016 Step Down Buck DC DC ConverterDokument7 SeitenXL4016 Step Down Buck DC DC ConverterCésar Fernando Rueda PortillaNoch keine Bewertungen
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDokument69 Seiten2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNoch keine Bewertungen
- IBRO News 2004Dokument8 SeitenIBRO News 2004International Brain Research Organization100% (1)
- MPDFDokument5 SeitenMPDFRoyalAryansNoch keine Bewertungen
- Inventory of Flood Bund PunjabDokument26 SeitenInventory of Flood Bund PunjabguildkeyNoch keine Bewertungen
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductVon EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductBewertung: 5 von 5 Sternen5/5 (31)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildVon EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildBewertung: 3.5 von 5 Sternen3.5/5 (9)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryVon EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNoch keine Bewertungen
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicVon EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNoch keine Bewertungen
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionVon EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousVon EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousBewertung: 5 von 5 Sternen5/5 (22)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryVon EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryBewertung: 5 von 5 Sternen5/5 (47)
- We Are the Luckiest: The Surprising Magic of a Sober LifeVon EverandWe Are the Luckiest: The Surprising Magic of a Sober LifeBewertung: 5 von 5 Sternen5/5 (183)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsVon EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNoch keine Bewertungen
- Easyway Express: Stop Smoking and Quit E-CigarettesVon EverandEasyway Express: Stop Smoking and Quit E-CigarettesBewertung: 5 von 5 Sternen5/5 (15)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingVon EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingBewertung: 5 von 5 Sternen5/5 (11)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineVon EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNoch keine Bewertungen
- Guts: The Endless Follies and Tiny Triumphs of a Giant DisasterVon EverandGuts: The Endless Follies and Tiny Triumphs of a Giant DisasterBewertung: 4 von 5 Sternen4/5 (99)
- Stop Drinking Now: The original Easyway methodVon EverandStop Drinking Now: The original Easyway methodBewertung: 5 von 5 Sternen5/5 (29)
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsVon EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsBewertung: 4.5 von 5 Sternen4.5/5 (6)
- Deaths of Despair and the Future of CapitalismVon EverandDeaths of Despair and the Future of CapitalismBewertung: 4.5 von 5 Sternen4.5/5 (30)
- Intoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingVon EverandIntoxicating Lies: One Woman’s Journey to Freedom from Gray Area DrinkingBewertung: 5 von 5 Sternen5/5 (1)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholVon EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholBewertung: 4 von 5 Sternen4/5 (6)
- The Complete ACOA Sourcebook: Adult Children of Alcoholics at Home, at Work and in LoveVon EverandThe Complete ACOA Sourcebook: Adult Children of Alcoholics at Home, at Work and in LoveBewertung: 5 von 5 Sternen5/5 (1)
- Living Sober: Practical methods alcoholics have used for living without drinkingVon EverandLiving Sober: Practical methods alcoholics have used for living without drinkingBewertung: 4 von 5 Sternen4/5 (50)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerVon EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerBewertung: 5 von 5 Sternen5/5 (8)
- Dopamine Detox: How Dopamine Detox Can Help You Take Control of Your Life (Reduce Instant Gratification Beat Social Media Addiction and Stop Wasting Your Life)Von EverandDopamine Detox: How Dopamine Detox Can Help You Take Control of Your Life (Reduce Instant Gratification Beat Social Media Addiction and Stop Wasting Your Life)Noch keine Bewertungen