Das könnte Ihnen auch gefallen
- Daniel Saladas ResumeDokument2 SeitenDaniel Saladas ResumeAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Application Forms (Fillable)Dokument2 SeitenApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- CV 2023010319584829Dokument1 SeiteCV 2023010319584829Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- Nursing Notes Maternal and Child Nursing CareDokument70 SeitenNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Credential Verification Form Non-Clinical (Without Signature Page)Dokument1 SeiteCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- FNCP PoorsanitationmarwahDokument3 SeitenFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- To Fill-Up Id-Atm FormDokument7 SeitenTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Poor Environmetal Sanitation As Health Threat CuesDokument11 SeitenPoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case Study PresentationDokument1 SeiteFamily Case Study PresentationAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Pnle ReviewerDokument293 SeitenPnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- Poor Compliance With Treatment As Health Threat CuesDokument11 SeitenPoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Health Teaching Plan FinaleDokument4 SeitenHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahNoch keine Bewertungen
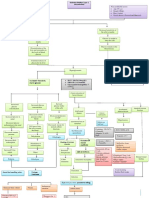
- Concept Map AtekharlssDokument3 SeitenConcept Map AtekharlssAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Water RescueDokument7 SeitenWater RescueAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case Study On Pulmonary TuberculosisDokument4 SeitenFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case StudyDokument33 SeitenFamily Case StudyAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Mock ResumeDokument3 SeitenMock ResumeAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Health EDUC Teaching Demo RubricsDokument4 SeitenHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDokument6 SeitenOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- History: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentDokument4 SeitenHistory: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDokument1 SeiteProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahNoch keine Bewertungen
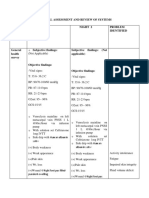
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDokument9 SeitenPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDokument12 SeitenAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Final Nursing CareplanDokument7 SeitenFinal Nursing CareplanAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationDokument11 SeitenAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Psychiatric-Mental Health NursingDokument6 SeitenPsychiatric-Mental Health NursingAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Post-Lecture Exam - Parasitology Answer KeyDokument87 SeitenPost-Lecture Exam - Parasitology Answer KeylenvycahpdelusaNoch keine Bewertungen
- Medicina Chinesa JeremyDokument2 SeitenMedicina Chinesa JeremyJuan Gabriel CunhaNoch keine Bewertungen
- Case StudyDokument3 SeitenCase StudyLouel VicitacionNoch keine Bewertungen
- On and Off Male Birth Control MethodsDokument2 SeitenOn and Off Male Birth Control MethodsLeón L.PNoch keine Bewertungen
- D An Introduction: Physical Medicine and RehabilitationDokument33 SeitenD An Introduction: Physical Medicine and RehabilitationChadNoch keine Bewertungen
- Knowledge, Attitude and Practices Towards Breast Feeding Among Lactating Mothers in King George Hospital, A Tertiary Care CenterDokument10 SeitenKnowledge, Attitude and Practices Towards Breast Feeding Among Lactating Mothers in King George Hospital, A Tertiary Care CenterIJAR JOURNALNoch keine Bewertungen
- IDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFDokument152 SeitenIDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFVivek KhakharNoch keine Bewertungen
- Newborn CareDokument19 SeitenNewborn CareYa Mei LiNoch keine Bewertungen
- Semi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniDokument7 SeitenSemi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniUmar FarooqNoch keine Bewertungen
- COMPLICATII TARDIVE DUPA INJECTAREA DE ACID HIALURONIC IN SCOP ESTETIC SI MANAGEMENTUL LOR Ro 399Dokument21 SeitenCOMPLICATII TARDIVE DUPA INJECTAREA DE ACID HIALURONIC IN SCOP ESTETIC SI MANAGEMENTUL LOR Ro 399tzupel4Noch keine Bewertungen
- Tercera SemanaDokument9 SeitenTercera SemanaJesús Torres MayaNoch keine Bewertungen
- HOẰNG HÓA 4-THANH HÓA 2022Dokument6 SeitenHOẰNG HÓA 4-THANH HÓA 2022Tuấn KhanhNoch keine Bewertungen
- Kleptomania Term PaperDokument6 SeitenKleptomania Term Paperbctfnerif100% (1)
- Extravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsDokument12 SeitenExtravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsmarcNoch keine Bewertungen
- John Leung, MD: Have You Brought With You The Following?Dokument3 SeitenJohn Leung, MD: Have You Brought With You The Following?Andres ANoch keine Bewertungen
- NCPDokument2 SeitenNCPfierfizNoch keine Bewertungen
- Glaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionDokument9 SeitenGlaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionFranco Paolo Maray-GhigliottoNoch keine Bewertungen
- The Aao "At-A-Glance" Guide To CDT 2021 Orthodontic Codes: DentitionDokument2 SeitenThe Aao "At-A-Glance" Guide To CDT 2021 Orthodontic Codes: DentitionSweet ToothNoch keine Bewertungen
- Guia NICE 2011 AutismoDokument51 SeitenGuia NICE 2011 Autismomecho9002Noch keine Bewertungen
- Treating Canine Distemper VirusDokument23 SeitenTreating Canine Distemper VirusJack HollandNoch keine Bewertungen
- Anesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFDokument125 SeitenAnesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFKatarina SimicicNoch keine Bewertungen
- Essential Oils Pocket Reference - Fifth EditionDokument206 SeitenEssential Oils Pocket Reference - Fifth Editionbianca7893% (88)
- Tolak Angin TranslatedDokument3 SeitenTolak Angin TranslatedWadz MuharNoch keine Bewertungen
- APA Practice Guideline For The Treatment of Patients With Substance Use DisordersDokument276 SeitenAPA Practice Guideline For The Treatment of Patients With Substance Use DisordersRaja Ahmad Rusdan MusyawirNoch keine Bewertungen
- Columbia Asia Referral HospitalDokument9 SeitenColumbia Asia Referral HospitalNeerajNoch keine Bewertungen
- McWilliams Center For Counseling, Inc. Community Support Office - 438Dokument2 SeitenMcWilliams Center For Counseling, Inc. Community Support Office - 438James BennettNoch keine Bewertungen
- Hospital Outpatient Prospective Payment System 2019 Updates - Shared1Dokument112 SeitenHospital Outpatient Prospective Payment System 2019 Updates - Shared1Nunya BiznesNoch keine Bewertungen
- Case Study On Acute PyelonephritisDokument85 SeitenCase Study On Acute Pyelonephritissanutulsi100% (23)
- Congestion Pelvica 2020Dokument6 SeitenCongestion Pelvica 2020Cristian RodríguezNoch keine Bewertungen