Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Pnle ReviewerDokument293 SeitenPnle ReviewerAsniah Hadjiadatu Abdullah94% (18)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- COLLOIDAL GOLD RECIPE - CitrateDokument9 SeitenCOLLOIDAL GOLD RECIPE - CitrateDevon Narok100% (4)
- Health EDUC Teaching Demo RubricsDokument4 SeitenHealth EDUC Teaching Demo RubricsAsniah Hadjiadatu Abdullah100% (1)
- B028-Sayli Kapse B029-Surya Teja B030-Taranum Kaur B032-Yashesh Kothari B034-Sathish Kumar B035-ManeeshDokument24 SeitenB028-Sayli Kapse B029-Surya Teja B030-Taranum Kaur B032-Yashesh Kothari B034-Sathish Kumar B035-ManeeshTaranum RandhawaNoch keine Bewertungen
- Service Manual - DM0412SDokument11 SeitenService Manual - DM0412SStefan Jovanovic100% (1)
- Nursing Care Plan ConstipationDokument3 SeitenNursing Care Plan Constipationbmrose3783% (12)
- Linkage 2 Lab ReportDokument25 SeitenLinkage 2 Lab Reportapi-25176084883% (6)
- Credential Verification Form Non-Clinical (Without Signature Page)Dokument1 SeiteCredential Verification Form Non-Clinical (Without Signature Page)Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- Daniel Saladas ResumeDokument2 SeitenDaniel Saladas ResumeAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- CV 2023010319584829Dokument1 SeiteCV 2023010319584829Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- Application Forms (Fillable)Dokument2 SeitenApplication Forms (Fillable)Asniah Hadjiadatu AbdullahNoch keine Bewertungen
- To Fill-Up Id-Atm FormDokument7 SeitenTo Fill-Up Id-Atm FormAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- FNCP PoorsanitationmarwahDokument3 SeitenFNCP PoorsanitationmarwahAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Health Teaching Plan FinaleDokument4 SeitenHealth Teaching Plan FinaleAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Nursing Notes Maternal and Child Nursing CareDokument70 SeitenNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case Study PresentationDokument1 SeiteFamily Case Study PresentationAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Poor Environmetal Sanitation As Health Threat CuesDokument11 SeitenPoor Environmetal Sanitation As Health Threat CuesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Water RescueDokument7 SeitenWater RescueAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case StudyDokument33 SeitenFamily Case StudyAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Family Case Study On Pulmonary TuberculosisDokument4 SeitenFamily Case Study On Pulmonary TuberculosisAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Or/Dr/Nicu/Pacu Requirements: Open Wound TypesDokument6 SeitenOr/Dr/Nicu/Pacu Requirements: Open Wound TypesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Poor Compliance With Treatment As Health Threat CuesDokument11 SeitenPoor Compliance With Treatment As Health Threat CuesAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Mock ResumeDokument3 SeitenMock ResumeAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- History: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentDokument4 SeitenHistory: Ebolavirus. After This Discovery, Scientists Concluded That The Virus Came From Two DifferentAsniah Hadjiadatu AbdullahNoch keine Bewertungen
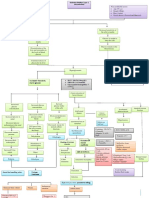
- Concept Map AtekharlssDokument3 SeitenConcept Map AtekharlssAsniah Hadjiadatu AbdullahNoch keine Bewertungen
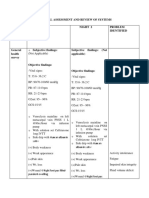
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDokument9 SeitenPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Proposed Budget For The 17th Striping and Pinning Investiture CeremonyDokument1 SeiteProposed Budget For The 17th Striping and Pinning Investiture CeremonyAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Assessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationDokument11 SeitenAssessment Nursing Diagnosis Planning (Desired or Expected Outcomes) Nursing Interventions Rationale EvaluationAsniah Hadjiadatu Abdullah100% (1)
- Assessments Nursing Diagnosis Planning Interventions Rationale EvaluationDokument12 SeitenAssessments Nursing Diagnosis Planning Interventions Rationale EvaluationAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Psychiatric-Mental Health NursingDokument6 SeitenPsychiatric-Mental Health NursingAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Final Nursing CareplanDokument7 SeitenFinal Nursing CareplanAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Biomedical EngineeringDokument5 SeitenBiomedical EngineeringFranch Maverick Arellano Lorilla100% (1)
- Aphids and Ants, Mutualistic Species, Share A Mariner Element With An Unusual Location On Aphid Chromosomes - PMCDokument2 SeitenAphids and Ants, Mutualistic Species, Share A Mariner Element With An Unusual Location On Aphid Chromosomes - PMC2aliciast7Noch keine Bewertungen
- LAB ActivityDokument2 SeitenLAB ActivityNicole AquinoNoch keine Bewertungen
- Naming Alcohols, Aldehydes. EtcDokument1 SeiteNaming Alcohols, Aldehydes. Etcim_mikezNoch keine Bewertungen
- CW Catalogue Cables and Wires A4 En-2Dokument1.156 SeitenCW Catalogue Cables and Wires A4 En-2Ovidiu PuieNoch keine Bewertungen
- Energies: Numerical Simulations On The Application of A Closed-Loop Lake Water Heat Pump System in The Lake Soyang, KoreaDokument16 SeitenEnergies: Numerical Simulations On The Application of A Closed-Loop Lake Water Heat Pump System in The Lake Soyang, KoreaMvikeli DlaminiNoch keine Bewertungen
- Jis C 8156-2017, EngDokument32 SeitenJis C 8156-2017, Eng7620383tlNoch keine Bewertungen
- SCL NotesDokument4 SeitenSCL NotesmayaNoch keine Bewertungen
- Adhi Wardana 405120042: Blok PenginderaanDokument51 SeitenAdhi Wardana 405120042: Blok PenginderaanErwin DiprajaNoch keine Bewertungen
- Excerpts From Roe v. Wade Majority OpinionDokument2 SeitenExcerpts From Roe v. Wade Majority OpinioncatherinewangcNoch keine Bewertungen
- Achievement Test Science 4 Regular ClassDokument9 SeitenAchievement Test Science 4 Regular ClassJassim MagallanesNoch keine Bewertungen
- הרצאה- אנמיה וטרומבוציטופניהDokument87 Seitenהרצאה- אנמיה וטרומבוציטופניהliatfurmanNoch keine Bewertungen
- 13 Unit 5 PainDokument4 Seiten13 Unit 5 PainAndres SalazarNoch keine Bewertungen
- Rekapan Belanja JKNDokument5 SeitenRekapan Belanja JKNAPOTEK PUSKESMAS MALEBERNoch keine Bewertungen
- Man Wah Ranked As Top 10 Furniture Sources For U.S. MarketDokument2 SeitenMan Wah Ranked As Top 10 Furniture Sources For U.S. MarketWeR1 Consultants Pte LtdNoch keine Bewertungen
- The Nursing ShortageDokument6 SeitenThe Nursing Shortageapi-455495817Noch keine Bewertungen
- PROJECT PROPOSAL AND PROJECT MANAGEMENT TOOLS GROUPWORK (Situation No. 3 - BSSW 3A)Dokument21 SeitenPROJECT PROPOSAL AND PROJECT MANAGEMENT TOOLS GROUPWORK (Situation No. 3 - BSSW 3A)Hermida Julia AlexandreaNoch keine Bewertungen
- Business-Plan (John Lloyd A Perido Grade 12-Arc)Dokument4 SeitenBusiness-Plan (John Lloyd A Perido Grade 12-Arc)Jaypher PeridoNoch keine Bewertungen
- C 08 S 09Dokument8 SeitenC 08 S 09Marnel Roy MayorNoch keine Bewertungen
- Student ChecklistDokument9 SeitenStudent Checklistapi-251493243Noch keine Bewertungen
- NACH FormDokument2 SeitenNACH FormShreyas WaghmareNoch keine Bewertungen
- Narrative Pathophysiology of PregnancyDokument2 SeitenNarrative Pathophysiology of PregnancyMarvin ChulyaoNoch keine Bewertungen
- Information Technology Solutions: ADMET Testing SystemsDokument2 SeitenInformation Technology Solutions: ADMET Testing Systemskrishgen biosystemsNoch keine Bewertungen
- Group 13Dokument4 SeitenGroup 13Surisetti Jyothsna LathaNoch keine Bewertungen
- 134.4902.06 - DM4170 - DatasheetDokument7 Seiten134.4902.06 - DM4170 - DatasheetVinicius MollNoch keine Bewertungen