Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Medical ManagerDokument336 SeitenMedical ManagerBatraneluNoch keine Bewertungen
- Catalog Statistica INSSE 2017 PDFDokument130 SeitenCatalog Statistica INSSE 2017 PDFBatraneluNoch keine Bewertungen
- Epidemiology and Fundamentals of Infectious DiseasesDokument308 SeitenEpidemiology and Fundamentals of Infectious DiseasesMr. Pushparaj Ghodke50% (2)
- Pitch - Neural Coding and Perception - C. Plack, Et Al., (Springer, 2005) WWDokument375 SeitenPitch - Neural Coding and Perception - C. Plack, Et Al., (Springer, 2005) WWBatranelu100% (1)
- World MalariaDokument238 SeitenWorld MalariadebugevdoNoch keine Bewertungen
- US Army Medical Course MD0589-100 - Environmental Injuries-Diseases IIDokument79 SeitenUS Army Medical Course MD0589-100 - Environmental Injuries-Diseases IIGeorgesNoch keine Bewertungen
- Healthcare Ethics IIDokument202 SeitenHealthcare Ethics IIApril ShowersNoch keine Bewertungen
- Army Soldier Health MaintinanceDokument103 SeitenArmy Soldier Health MaintinancePlainNormalGuy2100% (2)
- Army Soldier Health MaintinanceDokument103 SeitenArmy Soldier Health MaintinancePlainNormalGuy2100% (2)
- Us Army Medical BacteriologyDokument265 SeitenUs Army Medical BacteriologyPlainNormalGuy2Noch keine Bewertungen
- Pituitary Surgery - A Modern Approach - E. Laws, J. Sheehan (Karger, 2006) WW PDFDokument297 SeitenPituitary Surgery - A Modern Approach - E. Laws, J. Sheehan (Karger, 2006) WW PDFBatraneluNoch keine Bewertungen
- Computer Literacy IDokument124 SeitenComputer Literacy IApril ShowersNoch keine Bewertungen
- Army Soldier Health MaintinanceDokument103 SeitenArmy Soldier Health MaintinancePlainNormalGuy2100% (2)
- Us Army CC Md0574 Surgical MethodsDokument96 SeitenUs Army CC Md0574 Surgical MethodsRobert ButtsNoch keine Bewertungen
- Placenta and Trophoblast - Methods and Protocols (Vol 2) - M. Soares, J. Hunt (Humana, 2006) WW PDFDokument476 SeitenPlacenta and Trophoblast - Methods and Protocols (Vol 2) - M. Soares, J. Hunt (Humana, 2006) WW PDFBatraneluNoch keine Bewertungen
- Interpretarea Ritmului CardiacDokument40 SeitenInterpretarea Ritmului CardiacBatraneluNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- C# CodeDokument25 SeitenC# CodeKathryn MorrisonNoch keine Bewertungen
- By Phase - PlanningDokument60 SeitenBy Phase - Planningsyed rahmanNoch keine Bewertungen
- Examiners ' Comments and Key Points: FEEDBACK To Candidates June 2015 Part A ExaminationDokument31 SeitenExaminers ' Comments and Key Points: FEEDBACK To Candidates June 2015 Part A ExaminationsubiovefrigidoNoch keine Bewertungen
- How - To - Perform - An - Environmental - Management - Cost - AsDokument21 SeitenHow - To - Perform - An - Environmental - Management - Cost - AsTed TeddyNoch keine Bewertungen
- BDRRM plan-TEMPLATE 2020Dokument42 SeitenBDRRM plan-TEMPLATE 2020John Arbrith Isip Esposo100% (2)
- RP 44-7 Plant Layout: February 1996Dokument42 SeitenRP 44-7 Plant Layout: February 1996ridhwanmh100% (1)
- Question and Answer Igc2 Chapter 1 and 2Dokument20 SeitenQuestion and Answer Igc2 Chapter 1 and 2RahulNoch keine Bewertungen
- Icici Bank Project ReportDokument71 SeitenIcici Bank Project ReportGautam KumarNoch keine Bewertungen
- Best Practices Risk Mapping RR 07 01 04 PDFDokument4 SeitenBest Practices Risk Mapping RR 07 01 04 PDFVitalis MutsimbaNoch keine Bewertungen
- Auditing Manual Volume IDokument48 SeitenAuditing Manual Volume IElena PanainteNoch keine Bewertungen
- Medical Aspects of Fitness For Work Offshore - Guidance For Examining PhysiciansDokument80 SeitenMedical Aspects of Fitness For Work Offshore - Guidance For Examining PhysiciansJamie Taylor100% (6)
- Business Analytics For Project Management: Risk in The Project UndertakenDokument3 SeitenBusiness Analytics For Project Management: Risk in The Project UndertakenjeganathanNoch keine Bewertungen
- Risk Management Strategies Via Minimax Portfolio OptimizationDokument12 SeitenRisk Management Strategies Via Minimax Portfolio OptimizationJordan TaleskiNoch keine Bewertungen
- Online EN 120307 Napo Teachers Lesson3 pt1 HW PDFDokument9 SeitenOnline EN 120307 Napo Teachers Lesson3 pt1 HW PDFDA MARIA VLOGNoch keine Bewertungen
- Hamza - EntreDokument15 SeitenHamza - EntreAnas InamNoch keine Bewertungen
- Safe MooringDokument50 SeitenSafe MooringConselho Nacional de Praticagem100% (1)
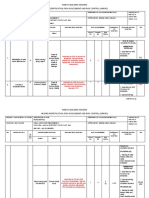
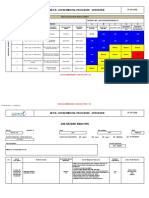
- Audit Objectives Procedures Evidences and DocumentationDokument35 SeitenAudit Objectives Procedures Evidences and Documentationrietzhel22100% (3)
- BTD Quality System Policy ManualDokument19 SeitenBTD Quality System Policy ManualPinaki DasNoch keine Bewertungen
- Cisco - SAFE Security Reference Architecture White PaperDokument9 SeitenCisco - SAFE Security Reference Architecture White PaperKhánh DuyNoch keine Bewertungen
- Introduction SLAuS 200Dokument24 SeitenIntroduction SLAuS 200naveen pragash100% (1)
- Glaciers Melting A Serious Threat To The Mountain Community of Gilgit BaltistanDokument2 SeitenGlaciers Melting A Serious Threat To The Mountain Community of Gilgit Baltistansadam khanNoch keine Bewertungen
- Helix Bond - Privilidge - Wealth PDFDokument12 SeitenHelix Bond - Privilidge - Wealth PDFhyenadogNoch keine Bewertungen
- Incepetion Report Organized Final 27-04-2021Dokument39 SeitenIncepetion Report Organized Final 27-04-2021DagimNoch keine Bewertungen
- SPC HIRADC - 022 - Road WorksDokument5 SeitenSPC HIRADC - 022 - Road WorksKalai ArasanNoch keine Bewertungen
- Fire Station PlanDokument6 SeitenFire Station PlanemmettoconnellNoch keine Bewertungen
- Review of Literature Empirical Research On Corporate GovernanceDokument5 SeitenReview of Literature Empirical Research On Corporate GovernanceaflsjizafNoch keine Bewertungen
- Motor Vehicle Showroom: Example Risk Assessment For ADokument3 SeitenMotor Vehicle Showroom: Example Risk Assessment For AOmar HfcNoch keine Bewertungen
- Delivery Considerations - A Report For HS2Dokument60 SeitenDelivery Considerations - A Report For HS2HighSpeedRail100% (1)
- Agribusiness Risk ManagementDokument34 SeitenAgribusiness Risk Managementdineshjain11Noch keine Bewertungen
- 29-JHA For Removal of Wooden PalletDokument4 Seiten29-JHA For Removal of Wooden PalletPradip Kumar ShaNoch keine Bewertungen