Das könnte Ihnen auch gefallen
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)Von EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)Noch keine Bewertungen
- RX in Pediatric DentistryDokument34 SeitenRX in Pediatric DentistryMohammed AlhayaniNoch keine Bewertungen
- Corrected MB MED LIST 2008Dokument2 SeitenCorrected MB MED LIST 2008tennillegoreNoch keine Bewertungen
- JAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatDokument3 SeitenJAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatJeraldeen JambalosNoch keine Bewertungen
- Sedation Reading TestDokument22 SeitenSedation Reading TestJyothy AthulNoch keine Bewertungen
- Paediatric Guidelines Croup 2020Dokument4 SeitenPaediatric Guidelines Croup 2020nimraNoch keine Bewertungen
- Drug-Induced Sleep Endoscopy (DISE)Dokument4 SeitenDrug-Induced Sleep Endoscopy (DISE)Luis De jesus SolanoNoch keine Bewertungen
- Week 7 Course TaskDokument13 SeitenWeek 7 Course TaskRachelle CambaNoch keine Bewertungen
- Material, Vincent M. (Types of Anesthesia Used in Cesarean Section)Dokument22 SeitenMaterial, Vincent M. (Types of Anesthesia Used in Cesarean Section)Vincent Maralit MaterialNoch keine Bewertungen
- COVID19 Management Algorithm 22042021 v1Dokument1 SeiteCOVID19 Management Algorithm 22042021 v1shivani shindeNoch keine Bewertungen
- BCCH ED Croup Algorithm 2012Dokument1 SeiteBCCH ED Croup Algorithm 2012john morzNoch keine Bewertungen
- Behaviour Management 2Dokument59 SeitenBehaviour Management 2Nikhil RaiNoch keine Bewertungen
- Anaphylaxis Wallchart 2018Dokument1 SeiteAnaphylaxis Wallchart 2018simranNoch keine Bewertungen
- Anaphylaxis Wallchart 2022Dokument1 SeiteAnaphylaxis Wallchart 2022Aymane El KandoussiNoch keine Bewertungen
- New Singulair MontelukastDokument1 SeiteNew Singulair MontelukastCassie100% (2)
- Er DrugsDokument15 SeitenEr DrugsDays AniarNoch keine Bewertungen
- FluticasoneDokument4 SeitenFluticasonevanNoch keine Bewertungen
- COVID Management 17th January 2022 DR Suvrankar Datta AIIMSDokument1 SeiteCOVID Management 17th January 2022 DR Suvrankar Datta AIIMSWhiteNoch keine Bewertungen
- COVID Clinical Management 14012022Dokument1 SeiteCOVID Clinical Management 14012022Naina DesaiNoch keine Bewertungen
- Pediatric Status Epilepticus CPGDokument7 SeitenPediatric Status Epilepticus CPGAndriNoch keine Bewertungen
- AtroventDokument2 SeitenAtroventKatie McPeekNoch keine Bewertungen
- Anaphylaxis & Allergic Reactions GuideDokument2 SeitenAnaphylaxis & Allergic Reactions Guidemadimadi11Noch keine Bewertungen
- Syok Anafilaksis 1Dokument4 SeitenSyok Anafilaksis 1Mariatun Zahro NasutionNoch keine Bewertungen
- Stress Steroid Management For Children With Primary or Secondary Adrenal FailureDokument5 SeitenStress Steroid Management For Children With Primary or Secondary Adrenal FailureGhada ElhassanNoch keine Bewertungen
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDokument1 SeiteAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Noch keine Bewertungen
- Faeldonea, PJ - Drug StudyDokument4 SeitenFaeldonea, PJ - Drug StudyPatricia Jean FaeldoneaNoch keine Bewertungen
- 8 Propofol Drug StudyDokument4 Seiten8 Propofol Drug Studyshadow gonzalez100% (1)
- Status Epilepticus Pediatric DR - RPDokument4 SeitenStatus Epilepticus Pediatric DR - RPAdnin NugrohoNoch keine Bewertungen
- Anaph 5Dokument7 SeitenAnaph 5Aprilihardini Laksmi100% (1)
- SedationDokument20 SeitenSedationelztly4694Noch keine Bewertungen
- Dr. Rajendra Prasad Koduri Specialist - Dept. of Anesthesia Mafraq Hospital. Review Article From The European Journal of Anesthesiology-EJA September 2008Dokument20 SeitenDr. Rajendra Prasad Koduri Specialist - Dept. of Anesthesia Mafraq Hospital. Review Article From The European Journal of Anesthesiology-EJA September 2008Kamal MohamedNoch keine Bewertungen
- Drug Study - SalbutamolDokument2 SeitenDrug Study - SalbutamolryanNoch keine Bewertungen
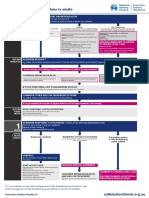
- Managing Acute Asthma in Adults - Final160123Dokument1 SeiteManaging Acute Asthma in Adults - Final160123Stri LokaNoch keine Bewertungen
- FentanylDokument2 SeitenFentanylKatie McPeek63% (8)
- Buotan Si June Buotan Jud Si JuneDokument13 SeitenBuotan Si June Buotan Jud Si JuneMajestic RavenNoch keine Bewertungen
- When To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsDokument9 SeitenWhen To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsepraetorianNoch keine Bewertungen
- Fentanyl NeomedDokument3 SeitenFentanyl NeomedmuarifNoch keine Bewertungen
- Atracurium BesylateDokument3 SeitenAtracurium BesylateWidya WidyariniNoch keine Bewertungen
- EpinephrineDokument4 SeitenEpinephrinegovind_soni_15Noch keine Bewertungen
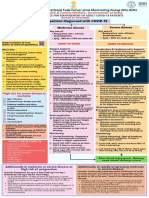
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDokument1 SeiteAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845Noch keine Bewertungen
- TRAMADOLDokument2 SeitenTRAMADOLchristine mercadoNoch keine Bewertungen
- Pharmacological Methods of Behaviour ManagementDokument41 SeitenPharmacological Methods of Behaviour ManagementSuma 123Noch keine Bewertungen
- Rabbit Formulary: Inhalation AnestheticsDokument3 SeitenRabbit Formulary: Inhalation AnestheticsMiriam CervantesNoch keine Bewertungen
- Drug Study - Colon CancerDokument4 SeitenDrug Study - Colon Cancerbea pegadNoch keine Bewertungen
- A Selective Summary of Psychopharmacology Research Published in First Half of 2017Dokument3 SeitenA Selective Summary of Psychopharmacology Research Published in First Half of 2017gion.nandNoch keine Bewertungen
- Medications: Medication Name Generic/Trade Classification Pregnancy CategoryDokument8 SeitenMedications: Medication Name Generic/Trade Classification Pregnancy CategoryapalestiNoch keine Bewertungen
- Myasthenia Gravis ReferatDokument26 SeitenMyasthenia Gravis ReferatUlfa TitiswariNoch keine Bewertungen
- XopenexDokument1 SeiteXopenexKatie McPeekNoch keine Bewertungen
- Algorithm - Managing A COPD Exacerbation in Primary CareDokument1 SeiteAlgorithm - Managing A COPD Exacerbation in Primary Caremufidah mawaddahNoch keine Bewertungen
- Advances in Feline AnesthesiaDokument5 SeitenAdvances in Feline AnesthesiaMabe AguirreNoch keine Bewertungen
- Evaluation and Management of Status Epilepticus in ChildrenDokument13 SeitenEvaluation and Management of Status Epilepticus in ChildrenAyan BiswasNoch keine Bewertungen
- Case Presentation Station 3B Drug Study ClinidineDokument6 SeitenCase Presentation Station 3B Drug Study ClinidinehahahahaaaaaaaNoch keine Bewertungen
- MC HydroxyzineDokument3 SeitenMC HydroxyzineCliff by the seaNoch keine Bewertungen
- DigoxinDokument2 SeitenDigoxinJulia TarlacNoch keine Bewertungen
- PHARMA LE1 Asthma & Cough Cram SheetDokument1 SeitePHARMA LE1 Asthma & Cough Cram SheetMarjorie MonesNoch keine Bewertungen
- AdrenalineDokument2 SeitenAdrenalinerazvan032006100% (1)
- Neonatal Medication Protocols: Drug: Salbutamol PresentationDokument1 SeiteNeonatal Medication Protocols: Drug: Salbutamol Presentationputra pratamaNoch keine Bewertungen
- She Drug StudyDokument23 SeitenShe Drug StudyShella DechavezNoch keine Bewertungen
- Librium ChlordiazepoxideDokument2 SeitenLibrium ChlordiazepoxideENoch keine Bewertungen
- Ventolin™ Nebules: Qualitative and Quantitative CompositionDokument8 SeitenVentolin™ Nebules: Qualitative and Quantitative CompositionnurfitriaNoch keine Bewertungen
- Ludwig'S Angina: A Case With A 5-Year Follow-Up: SciencedirectDokument6 SeitenLudwig'S Angina: A Case With A 5-Year Follow-Up: SciencedirectnurfitriaNoch keine Bewertungen
- Salbutamol 2017: Newborn Use OnlyDokument3 SeitenSalbutamol 2017: Newborn Use OnlynurfitriaNoch keine Bewertungen
- Nerve GlidingDokument11 SeitenNerve GlidingnurfitriaNoch keine Bewertungen
- Trom Bell I 2018Dokument28 SeitenTrom Bell I 2018nurfitriaNoch keine Bewertungen
- Gigi Dan MulutDokument6 SeitenGigi Dan MulutnurfitriaNoch keine Bewertungen
- Daftar Pustaka: (Medline)Dokument14 SeitenDaftar Pustaka: (Medline)nurfitriaNoch keine Bewertungen
- Seminar: Anders Hviid, Steven Rubin, Kathrin MühlemannDokument13 SeitenSeminar: Anders Hviid, Steven Rubin, Kathrin MühlemannnurfitriaNoch keine Bewertungen
- Aydin 2016Dokument5 SeitenAydin 2016nurfitriaNoch keine Bewertungen
- Adult Intussusception: An Institutional Experience and Review of LiteratureDokument6 SeitenAdult Intussusception: An Institutional Experience and Review of LiteraturenurfitriaNoch keine Bewertungen
- Methylphenidate and Dextroamphetamine Abuse in Substance-Abusing AdolescentsDokument14 SeitenMethylphenidate and Dextroamphetamine Abuse in Substance-Abusing AdolescentsnurfitriaNoch keine Bewertungen
- Lee2011 PDFDokument14 SeitenLee2011 PDFnurfitriaNoch keine Bewertungen
- Drug Abuse AdhdDokument12 SeitenDrug Abuse AdhdnurfitriaNoch keine Bewertungen
- Methylphenidate Amplifies The Potency and Reinforcing Effects of Amphetamines by Increasing Dopamine Transporter ExpressionDokument10 SeitenMethylphenidate Amplifies The Potency and Reinforcing Effects of Amphetamines by Increasing Dopamine Transporter ExpressionnurfitriaNoch keine Bewertungen
- Sugawara J Cath 2012Dokument7 SeitenSugawara J Cath 2012nurfitriaNoch keine Bewertungen
- Methylphenidate Doses in Attention de Ficit/ Hyperactivity Disorder and Comorbid Substance Use DisordersDokument9 SeitenMethylphenidate Doses in Attention de Ficit/ Hyperactivity Disorder and Comorbid Substance Use DisordersnurfitriaNoch keine Bewertungen
- Skoglund 2016Dokument7 SeitenSkoglund 2016nurfitriaNoch keine Bewertungen
- Volk Ow 2008Dokument4 SeitenVolk Ow 2008nurfitriaNoch keine Bewertungen
- IvermectinDokument9 SeitenIvermectinnurfitria100% (1)
- NYS OPWDD March 28th COVID-19 Protocol For Essential PersonnelDokument2 SeitenNYS OPWDD March 28th COVID-19 Protocol For Essential PersonnelLaw&CrimeNoch keine Bewertungen
- Appropiate Allergic Testing and The Interpretation - Dr. Deshinta Putri Mulya, SP - PD (K) KAIDokument40 SeitenAppropiate Allergic Testing and The Interpretation - Dr. Deshinta Putri Mulya, SP - PD (K) KAIEllenNoch keine Bewertungen
- Gastrointestinal Nursing ReviewDokument50 SeitenGastrointestinal Nursing ReviewRoby NgNoch keine Bewertungen
- Lung MycosisDokument80 SeitenLung MycosisWisnu Omadi100% (2)
- Medical SpecialistsDokument2 SeitenMedical SpecialistsArvin Dela CrÜzNoch keine Bewertungen
- Go Red For Women PresentationDokument31 SeitenGo Red For Women PresentationadithiNoch keine Bewertungen
- Respon Metabolik Sepsis - PPDS Igk FK - Undip (Ed)Dokument52 SeitenRespon Metabolik Sepsis - PPDS Igk FK - Undip (Ed)Indra WatiNoch keine Bewertungen
- Drug Study: Notre Dame of Tacurong CollegeDokument2 SeitenDrug Study: Notre Dame of Tacurong CollegeApol PenNoch keine Bewertungen
- Co-Occurring Disorders: Substance Use and Mental HealthDokument52 SeitenCo-Occurring Disorders: Substance Use and Mental HealthElisyah MarsiahNoch keine Bewertungen
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goals: Independent: Short Term GoalsDokument2 SeitenAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goals: Independent: Short Term GoalskyawNoch keine Bewertungen
- 01 - 3【English】 (Sample) Prevaccination Screening QuestionnaireDokument1 Seite01 - 3【English】 (Sample) Prevaccination Screening QuestionnaireThet Ko WinNoch keine Bewertungen
- MINDMAPDokument2 SeitenMINDMAPrayzaoliveira.ausNoch keine Bewertungen
- 5 курс Тема 12. (English translation)Dokument8 Seiten5 курс Тема 12. (English translation)Viktoriya GorobinskayaNoch keine Bewertungen
- Empiric Antibiotic ListDokument2 SeitenEmpiric Antibiotic ListpasswordNoch keine Bewertungen
- Vdoc - Pub End of Life Care in Cardiovascular DiseaseDokument251 SeitenVdoc - Pub End of Life Care in Cardiovascular Diseasericardo valtierra diaz infanteNoch keine Bewertungen
- Effects of Smoking & What Is Passive Smoking?Dokument9 SeitenEffects of Smoking & What Is Passive Smoking?天天Noch keine Bewertungen
- Oral Systemic Link Lesson Plan 2Dokument10 SeitenOral Systemic Link Lesson Plan 2api-543973374Noch keine Bewertungen
- CNS DrugsDokument57 SeitenCNS DrugsHussein Al-jmrawiNoch keine Bewertungen
- CBT Midwifery Full Mock Test 3 Questions Answers Numerical OrderDokument31 SeitenCBT Midwifery Full Mock Test 3 Questions Answers Numerical OrderMimi BoamahNoch keine Bewertungen
- Electrocardiogram: Dr. PacnaDokument13 SeitenElectrocardiogram: Dr. PacnaEcel AggasidNoch keine Bewertungen
- Drug Study (Schizo)Dokument5 SeitenDrug Study (Schizo)aliannaNoch keine Bewertungen
- Vascular Note by Joel ArudchelvamDokument52 SeitenVascular Note by Joel ArudchelvamJoel Arudchelvam100% (1)
- Family Structure Assessment:: GenogramDokument10 SeitenFamily Structure Assessment:: GenogramFlorentino Jr. TarucNoch keine Bewertungen
- Leukemia CaseDokument28 SeitenLeukemia CasehilalNoch keine Bewertungen
- Laparoscopic Correction of Perforated Peptic Ulcer First Choice A Review of LiteratureDokument9 SeitenLaparoscopic Correction of Perforated Peptic Ulcer First Choice A Review of LiteratureLe Hu ThaNoch keine Bewertungen
- FMGE July 2023 PrepLadder 1Dokument558 SeitenFMGE July 2023 PrepLadder 1Sahil AhlawatNoch keine Bewertungen
- Era University / Era College of Nursing: Lesson Plan On-Breast GynecomastiaDokument8 SeitenEra University / Era College of Nursing: Lesson Plan On-Breast GynecomastiaShreya SinhaNoch keine Bewertungen
- Pain Managment in Labor 2020Dokument5 SeitenPain Managment in Labor 2020António BragaNoch keine Bewertungen
- Aurora 2012Dokument7 SeitenAurora 2012Phạm Văn HiệpNoch keine Bewertungen
- Case On TrachomaDokument20 SeitenCase On Trachomadimple alluriNoch keine Bewertungen