Das könnte Ihnen auch gefallen
- Clinical Examination of The ShoulderDokument195 SeitenClinical Examination of The ShouldernikithaNoch keine Bewertungen
- Red Flags II. A Guide To Solving Serious Pathology of The Spine-Churchill Livingstone (2009)Dokument240 SeitenRed Flags II. A Guide To Solving Serious Pathology of The Spine-Churchill Livingstone (2009)Oana MozaNoch keine Bewertungen
- The CEO's Guide To The Generative AI Revolution - BCGDokument14 SeitenThe CEO's Guide To The Generative AI Revolution - BCGjm petit100% (1)
- PersuassionDokument25 SeitenPersuassionShan AliNoch keine Bewertungen
- Homeroom Guidance Program Grade 10 Agoho Module 1: Decoding The Secrets of Better Study HabitsDokument4 SeitenHomeroom Guidance Program Grade 10 Agoho Module 1: Decoding The Secrets of Better Study HabitsMathPad with Teacher Anabel100% (5)
- Benefits and Beneficiaries of ResearchDokument25 SeitenBenefits and Beneficiaries of ResearchELA REYESNoch keine Bewertungen
- Historical Journal Entry Rubricworld HistoryDokument2 SeitenHistorical Journal Entry Rubricworld Historyapi-241347803Noch keine Bewertungen
- Wrist and Ankle Acupuncture Book, by Josep CarrionDokument199 SeitenWrist and Ankle Acupuncture Book, by Josep Carrionjosep100% (2)
- Unit 1: Nursing ResearchDokument101 SeitenUnit 1: Nursing ResearchHardeep Kaur100% (1)
- Reviewer in PhilosophyDokument4 SeitenReviewer in PhilosophyEllie CastroNoch keine Bewertungen
- Northern Mindanao Colleges, Inc.: Outcomes - Based Course Syllabus Research 1Dokument5 SeitenNorthern Mindanao Colleges, Inc.: Outcomes - Based Course Syllabus Research 1Brian Reyes GangcaNoch keine Bewertungen
- Acupuncturist Perceptions of Serving As A Clinical Trial PractitionerDokument7 SeitenAcupuncturist Perceptions of Serving As A Clinical Trial Practitionerbinglei chenNoch keine Bewertungen
- Mills 2004Dokument8 SeitenMills 2004Tari RiyastiNoch keine Bewertungen
- Double-Blinding of An Acupuncture Randomized Controlled Trial Optimized With Clinical Translational Science Award ResourcesDokument7 SeitenDouble-Blinding of An Acupuncture Randomized Controlled Trial Optimized With Clinical Translational Science Award ResourcesSam SamNoch keine Bewertungen
- UGML JAMA - I - How To Get StartedDokument3 SeitenUGML JAMA - I - How To Get StartedAlicia WellmannNoch keine Bewertungen
- Nihms 1598987Dokument14 SeitenNihms 1598987Sam SamNoch keine Bewertungen
- A Simple Guide To Reading An: - HcspfactsheetDokument2 SeitenA Simple Guide To Reading An: - HcspfactsheetRinawati UnissulaNoch keine Bewertungen
- Vpe 006Dokument4 SeitenVpe 006Jailouise PerezNoch keine Bewertungen
- MAN ParaTitle-Manuscript - Grace-EpresDokument80 SeitenMAN ParaTitle-Manuscript - Grace-EpresSevered AppleheadNoch keine Bewertungen
- Teaching The Neurological Examination in A Rapidly Evolving Clinical ClimateDokument13 SeitenTeaching The Neurological Examination in A Rapidly Evolving Clinical Climatemh8m58brjnNoch keine Bewertungen
- Placebo EthicDokument12 SeitenPlacebo EthicHeQta SSNoch keine Bewertungen
- Eliciting Critical Care Nurses' Beliefs Regarding Physical Restraint UseDokument15 SeitenEliciting Critical Care Nurses' Beliefs Regarding Physical Restraint UseitaNoch keine Bewertungen
- Mosoiu Et Al 2023 Core Palliative Care Research Competencies Framework For Palliative Care CliniciansDokument10 SeitenMosoiu Et Al 2023 Core Palliative Care Research Competencies Framework For Palliative Care CliniciansAmbaNoch keine Bewertungen
- Clinical Reasoning Strategies in PTDokument19 SeitenClinical Reasoning Strategies in PTamitesh_mpthNoch keine Bewertungen
- An Overview of Clinical ResearchDokument5 SeitenAn Overview of Clinical ResearchDayanne Alexandra B.PNoch keine Bewertungen
- Week 3 Evidence Based NursingDokument4 SeitenWeek 3 Evidence Based NursingFrances BañezNoch keine Bewertungen
- AConciseGuidetoClinicalReasoning PrepublicationDokument23 SeitenAConciseGuidetoClinicalReasoning PrepublicationAlejandroNoch keine Bewertungen
- Etiquette-Based Medicine: PerspectiveDokument2 SeitenEtiquette-Based Medicine: PerspectiveTony Gomez Luna LeyvaNoch keine Bewertungen
- Error Detection and Recovery in Dialysis Nursing: Riginal RticleDokument11 SeitenError Detection and Recovery in Dialysis Nursing: Riginal RticleSilvalia RahmaNoch keine Bewertungen
- Como Hacer dx-1Dokument6 SeitenComo Hacer dx-1Krys Vargas DazaNoch keine Bewertungen
- Postmedj00208 0062cDokument2 SeitenPostmedj00208 0062cابراهيم العسيريNoch keine Bewertungen
- NeuroDokument16 SeitenNeurodavid.brieberNoch keine Bewertungen
- IntroductionDokument3 SeitenIntroductionAndrei BulgariuNoch keine Bewertungen
- Sessler, Methodology 1, Sources of ErrorDokument9 SeitenSessler, Methodology 1, Sources of ErrorMarcia Alvarez ZeballosNoch keine Bewertungen
- He Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceDokument7 SeitenHe Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceFrederico PóvoaNoch keine Bewertungen
- Journal Massage Untuk Bell PalsyDokument10 SeitenJournal Massage Untuk Bell PalsyauliyaNoch keine Bewertungen
- Sedation and Analgesia For Procedures in The Pediatric Emergency RoomDokument17 SeitenSedation and Analgesia For Procedures in The Pediatric Emergency Roomgv xdNoch keine Bewertungen
- Sedation and Analgesia For Procedur in The Pediatric Emergency RoomDokument17 SeitenSedation and Analgesia For Procedur in The Pediatric Emergency Roomfuka priesleyNoch keine Bewertungen
- Manejo EstreñimientolarkinDokument12 SeitenManejo EstreñimientolarkinJaimeNoch keine Bewertungen
- Clin Experimental Optometry - 2008 - Clinical Medicine in Optometric Practice 2nd EditionDokument2 SeitenClin Experimental Optometry - 2008 - Clinical Medicine in Optometric Practice 2nd EditionnicolamihaiuNoch keine Bewertungen
- Clinical Reasoning in Manual TherapyDokument11 SeitenClinical Reasoning in Manual TherapyKhushboo PakhraniNoch keine Bewertungen
- Pediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyDokument5 SeitenPediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyagusNoch keine Bewertungen
- 2006-Long-Term Use of Oxcarbazepine Oral Suspension in Childhood Epilepsy - Open-Label Study PDFDokument6 Seiten2006-Long-Term Use of Oxcarbazepine Oral Suspension in Childhood Epilepsy - Open-Label Study PDFAnonymous bEwTSXJ1gNoch keine Bewertungen
- Neurology Syllabus 2012-2013Dokument73 SeitenNeurology Syllabus 2012-2013kriskris12345Noch keine Bewertungen
- C P G: C C L B P: Riginal RticleDokument22 SeitenC P G: C C L B P: Riginal RticleRajender BishtNoch keine Bewertungen
- Therapeutic Nursing InterventionsDokument2 SeitenTherapeutic Nursing Interventionsapi-539369902Noch keine Bewertungen
- Single-Case Research Designs in Clinical Child Psychiatry: Journal of The American Academy of Child PsychiatryDokument10 SeitenSingle-Case Research Designs in Clinical Child Psychiatry: Journal of The American Academy of Child PsychiatryKarla SuárezNoch keine Bewertungen
- Principles of Evidence Based MedicineDokument16 SeitenPrinciples of Evidence Based MedicineDiego BeltranNoch keine Bewertungen
- Tugas Summary Artikel 2-DikonversiDokument10 SeitenTugas Summary Artikel 2-DikonversiAyu WulansariNoch keine Bewertungen
- 10.1055s 0039 1688815 - CompressedDokument15 Seiten10.1055s 0039 1688815 - CompressedYolanda Gómez LópezNoch keine Bewertungen
- Mejora de Validez en Investig Del Tratamiento de ComorbilidadDokument11 SeitenMejora de Validez en Investig Del Tratamiento de ComorbilidadDanitza YhovannaNoch keine Bewertungen
- PTRS SR FinalDokument27 SeitenPTRS SR FinalEloisa CellonaNoch keine Bewertungen
- Literature Review of Studies On The Effectiveness of Nurses Ability To Order and Interpret X-RaysDokument8 SeitenLiterature Review of Studies On The Effectiveness of Nurses Ability To Order and Interpret X-RaysFlorsie MirandaNoch keine Bewertungen
- Principles of Evidence Based MedicineDokument3 SeitenPrinciples of Evidence Based MedicineFernandaPelayoNoch keine Bewertungen
- Final Reflective JournalDokument2 SeitenFinal Reflective Journalapi-547582127Noch keine Bewertungen
- Clinical Reasoning: Linking Theory To Practice and Practice To TheoryDokument14 SeitenClinical Reasoning: Linking Theory To Practice and Practice To Theorylumac1087831Noch keine Bewertungen
- Barriers To Effective PARU Handover: ACORN December 2010Dokument6 SeitenBarriers To Effective PARU Handover: ACORN December 2010Pebri IrawanNoch keine Bewertungen
- Learning The Art and Science of Diagnosis - JAMADokument2 SeitenLearning The Art and Science of Diagnosis - JAMAJose Antonio Tous OlagortaNoch keine Bewertungen
- Critical Appraisal of An Article About TherapyDokument5 SeitenCritical Appraisal of An Article About TherapySheila Lyn LacsonNoch keine Bewertungen
- Epilepsy Research Paper ConclusionDokument7 SeitenEpilepsy Research Paper Conclusionzpyrufrif100% (1)
- Cyclosporine For Moderate-To-Severe Alopecia Areata: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial of Efficacy and SafetyDokument8 SeitenCyclosporine For Moderate-To-Severe Alopecia Areata: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial of Efficacy and Safetysupaidi97Noch keine Bewertungen
- Pauta Enuresis N&ADokument3 SeitenPauta Enuresis N&APedro Y. LuyoNoch keine Bewertungen
- Theaching Clinicla Medicine The Key Principals. Q J Med. 2015Dokument8 SeitenTheaching Clinicla Medicine The Key Principals. Q J Med. 2015Carolina Serna RojasNoch keine Bewertungen
- Clinical Reasoning 2Dokument10 SeitenClinical Reasoning 2Phooi Yee LauNoch keine Bewertungen
- Perioperative Homeopathic Arnica and BromelainDokument6 SeitenPerioperative Homeopathic Arnica and BromelainrachiddellarNoch keine Bewertungen
- Restraints in Dementia Care: A Nurse’s Guide to Minimizing Their UseVon EverandRestraints in Dementia Care: A Nurse’s Guide to Minimizing Their UseNoch keine Bewertungen
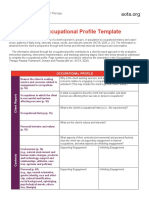
- AOTA Occupational Profile TemplateDokument2 SeitenAOTA Occupational Profile TemplateYayan100% (1)
- The New Evaluation Codes: What Are Performance Deficits?Dokument2 SeitenThe New Evaluation Codes: What Are Performance Deficits?YayanNoch keine Bewertungen
- ErgonomicsDokument2 SeitenErgonomicsYayanNoch keine Bewertungen
- Which Picture Is The Same?: Name - DateDokument6 SeitenWhich Picture Is The Same?: Name - DateYayanNoch keine Bewertungen
- Semantic Web-Module1Dokument75 SeitenSemantic Web-Module1Viji RajendranNoch keine Bewertungen
- Second Grade Science Matter Lesson Plan Liquids ObservationDokument3 SeitenSecond Grade Science Matter Lesson Plan Liquids Observationapi-236126271Noch keine Bewertungen
- Research AgendaDokument43 SeitenResearch AgendaArnel UsmanNoch keine Bewertungen
- Moral Theories and Ethical FrameworksDokument4 SeitenMoral Theories and Ethical FrameworksdirkdarrenNoch keine Bewertungen
- Assessing Metacognition in Children and AdultsDokument49 SeitenAssessing Metacognition in Children and AdultsJuliette100% (1)
- Multiclass Classification Method Based On Deep Learning For Leaf Identification For FarmersDokument4 SeitenMulticlass Classification Method Based On Deep Learning For Leaf Identification For FarmersInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- English Parts Uf Speech PDFDokument14 SeitenEnglish Parts Uf Speech PDFAnil SharmaNoch keine Bewertungen
- Writing A Comparison and Contrast EssayDokument24 SeitenWriting A Comparison and Contrast EssaycamilutNoch keine Bewertungen
- Second Quarter: Positive and Negative Messages Conveyed in ADokument3 SeitenSecond Quarter: Positive and Negative Messages Conveyed in AMACAINAG, AngelicaNoch keine Bewertungen
- Adverbs الحال PDFDokument15 SeitenAdverbs الحال PDFLearnEnglishESLNoch keine Bewertungen
- 2-Frustration ILMP-INDIVIDUAL-LEARNING-MONITORING-PLAN-FOR-ENRICHMENTDokument2 Seiten2-Frustration ILMP-INDIVIDUAL-LEARNING-MONITORING-PLAN-FOR-ENRICHMENTISABELO III ALFEREZNoch keine Bewertungen
- Villarreal Taylor Teaching ResumeDokument4 SeitenVillarreal Taylor Teaching Resumeapi-597260702Noch keine Bewertungen
- Forensics PTSD Presentation-ADokument34 SeitenForensics PTSD Presentation-AAndreas Paris100% (1)
- Evidente, J.D. g7 English May8 12Dokument9 SeitenEvidente, J.D. g7 English May8 12JoanEvidenteNoch keine Bewertungen
- EogDokument16 SeitenEogchoppersureNoch keine Bewertungen
- Curriculum ExperiencesDokument11 SeitenCurriculum ExperiencesMarvin VinasNoch keine Bewertungen
- New Curriculum Formative Assessment NCDCDokument26 SeitenNew Curriculum Formative Assessment NCDCRobert Kityo ProNoch keine Bewertungen
- Iep Case StudyDokument16 SeitenIep Case Studyapi-343163369Noch keine Bewertungen
- 1 IntroductionDokument72 Seiten1 IntroductionPratik Pradip SarodeNoch keine Bewertungen
- DCT Example Exercise Summary ReportDokument2 SeitenDCT Example Exercise Summary ReportprofessormcgillNoch keine Bewertungen
- Learning Compeencies Domain LC SS: Quarter 3Dokument4 SeitenLearning Compeencies Domain LC SS: Quarter 3Yasmin G. BaoitNoch keine Bewertungen
- Educ 202 Module Chapter 1 - 2Dokument18 SeitenEduc 202 Module Chapter 1 - 2Raymond MaristelaNoch keine Bewertungen
- Study The Job Satisfaction of Employees in SBI LTD 2Dokument51 SeitenStudy The Job Satisfaction of Employees in SBI LTD 2Ashish NavalNoch keine Bewertungen