Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Sexually Transmitted Disesase.: Ralph Gabriel QuinalDokument16 SeitenSexually Transmitted Disesase.: Ralph Gabriel QuinalJohn Michael MonteflacoNoch keine Bewertungen
- The-Sexual-Self LectureDokument109 SeitenThe-Sexual-Self LectureElaine Fiona VillafuerteNoch keine Bewertungen
- DEVPSYCH 12 - Psychosocial Development in AdolescenceDokument4 SeitenDEVPSYCH 12 - Psychosocial Development in AdolescenceRedgie G. GabaneNoch keine Bewertungen
- BRS Peds NotesDokument57 SeitenBRS Peds NotesRkkNoch keine Bewertungen
- Lesson 6Dokument13 SeitenLesson 6zeltonNoch keine Bewertungen
- Microbiology Viriology and ImmunologyDokument44 SeitenMicrobiology Viriology and ImmunologyRoseline AdebisiNoch keine Bewertungen
- Sexual Transmited DiseaseDokument74 SeitenSexual Transmited DiseaseAdi PeeNoch keine Bewertungen
- Vesicaria Communis John Henry Clarke: 21 Homeopathic Medicines Dr. Shah FaisalDokument3 SeitenVesicaria Communis John Henry Clarke: 21 Homeopathic Medicines Dr. Shah FaisalShah FaisalNoch keine Bewertungen
- A Case of Multiple Warts: Presented by Dr.K.Shiva Kumar, Ii M.D (Hom)Dokument41 SeitenA Case of Multiple Warts: Presented by Dr.K.Shiva Kumar, Ii M.D (Hom)Rahul PandeyNoch keine Bewertungen
- Medicare CMS Prevention QuickReferenceChart 1Dokument8 SeitenMedicare CMS Prevention QuickReferenceChart 1jpmed13Noch keine Bewertungen
- 10th Lecture (NCM 104 CD II) Care of Clients With Problems inDokument23 Seiten10th Lecture (NCM 104 CD II) Care of Clients With Problems inIcka Fong50% (4)
- LP Bacteria ChartDokument21 SeitenLP Bacteria ChartTaman HoangNoch keine Bewertungen
- Gonorrhoea Information and AdviceDokument9 SeitenGonorrhoea Information and AdviceNovel RamadhaniNoch keine Bewertungen
- Microbial Structures and Functions MoicroorganismsDokument390 SeitenMicrobial Structures and Functions MoicroorganismssamsoatsNoch keine Bewertungen
- Name of Infection/virus Acquired at What Time How To Test For It Likely S/s HSVDokument1 SeiteName of Infection/virus Acquired at What Time How To Test For It Likely S/s HSVC RNoch keine Bewertungen
- PerverseSpirit - Herb PohlmeyerDokument24 SeitenPerverseSpirit - Herb PohlmeyerNicole Victory50% (2)
- Chapter 24 HomeworkDokument9 SeitenChapter 24 HomeworkKvn4N6Noch keine Bewertungen
- Reading Hormonal Changes During PregnancyDokument6 SeitenReading Hormonal Changes During PregnancyKlinik Asy syifaNoch keine Bewertungen
- Determinant Factors That Influence The Prevalence of Gonorrhea in Female Sex Wokers in YogyakartaDokument12 SeitenDeterminant Factors That Influence The Prevalence of Gonorrhea in Female Sex Wokers in YogyakartaSiti MaesarohNoch keine Bewertungen
- Itch, Clap, Pox Venereal Disease in The Eighteenth-Century Imagination PDFDokument280 SeitenItch, Clap, Pox Venereal Disease in The Eighteenth-Century Imagination PDFtoadere100% (3)
- Midterm Module SocSci 111Dokument40 SeitenMidterm Module SocSci 111Frances Georgina FabaleNoch keine Bewertungen
- PHMDokument9 SeitenPHMPritib KumarNoch keine Bewertungen
- Health Related Fitness TestDokument6 SeitenHealth Related Fitness TestAimee HernandezNoch keine Bewertungen
- Trends & Treatment in STI Management in Primary Care - Dr. Salmiah ShariffDokument31 SeitenTrends & Treatment in STI Management in Primary Care - Dr. Salmiah ShariffhafizStudioNoch keine Bewertungen
- Philippine National AIDS Council & Take The Test Campaign, IncDokument41 SeitenPhilippine National AIDS Council & Take The Test Campaign, IncAngel Kate Salip BokNoch keine Bewertungen
- Post Coital BleedingDokument8 SeitenPost Coital BleedingMutiara SwNoch keine Bewertungen
- Section 9 - Students WorksheetDokument6 SeitenSection 9 - Students WorksheetEsraa AhmedNoch keine Bewertungen
- U.S. Selected Practice Recommendations For Contraceptive Use, 2016 MMWRDokument60 SeitenU.S. Selected Practice Recommendations For Contraceptive Use, 2016 MMWRhectorNoch keine Bewertungen
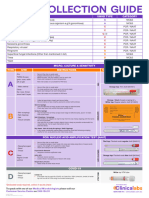
- Swab GuideDokument1 SeiteSwab GuideKarim SirNoch keine Bewertungen
- Microbial Diseases of The Urinary and Reproductive SystemsDokument139 SeitenMicrobial Diseases of The Urinary and Reproductive Systemsone_nd_onlyuNoch keine Bewertungen