Das könnte Ihnen auch gefallen
- Clifford Odets Paradise LostDokument21 SeitenClifford Odets Paradise LostEleftherios Anevlavis100% (2)
- Hypothetical State of Nature: Democracy The Legitimacy of GovernmentDokument10 SeitenHypothetical State of Nature: Democracy The Legitimacy of GovernmentEleftherios AnevlavisNoch keine Bewertungen
- Germaine de Staël and CorinneDokument7 SeitenGermaine de Staël and CorinneEleftherios AnevlavisNoch keine Bewertungen
- Metandmorefus Sed: Finnegans Wake As A Secret Agent? ... A FantasyDokument8 SeitenMetandmorefus Sed: Finnegans Wake As A Secret Agent? ... A FantasyEleftherios AnevlavisNoch keine Bewertungen
- A Tongue-In-Cheek Poem: - , "The Rose Family"Dokument1 SeiteA Tongue-In-Cheek Poem: - , "The Rose Family"Eleftherios AnevlavisNoch keine Bewertungen
- Hypermedia Joyce StudiesDokument2 SeitenHypermedia Joyce StudiesEleftherios AnevlavisNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Data Sheet: Permanent Magnet GeneratorDokument2 SeitenData Sheet: Permanent Magnet Generatordiegoadjgt100% (1)
- Medicinal Chemistry-Ii: 1.anti-Infective Agents: FDokument14 SeitenMedicinal Chemistry-Ii: 1.anti-Infective Agents: FAnonymous ionOPaqlkNoch keine Bewertungen
- Juniper M5 M10 DatasheetDokument6 SeitenJuniper M5 M10 DatasheetMohammed Ali ZainNoch keine Bewertungen
- FM - 30 MCQDokument8 SeitenFM - 30 MCQsiva sankarNoch keine Bewertungen
- PCIB Vs ESCOLIN (G.R. No. L-27860 & L-27896)Dokument61 SeitenPCIB Vs ESCOLIN (G.R. No. L-27860 & L-27896)strgrlNoch keine Bewertungen
- Influence of Intellectual Capital in The Organizational InnovationDokument8 SeitenInfluence of Intellectual Capital in The Organizational InnovationsopingiNoch keine Bewertungen
- People V NiellesDokument2 SeitenPeople V NiellesRobielyn Kate NerpioNoch keine Bewertungen
- David-Huynh Indeed ResumeDokument3 SeitenDavid-Huynh Indeed Resumeapi-546353822Noch keine Bewertungen
- Grammar WorksheetsDokument161 SeitenGrammar WorksheetsKhánhNoch keine Bewertungen
- Lucero Flores Resume 2Dokument2 SeitenLucero Flores Resume 2api-260292914Noch keine Bewertungen
- 06 BuyLog2013 MoldedCaseCircBrkrsDokument106 Seiten06 BuyLog2013 MoldedCaseCircBrkrsmarbyNoch keine Bewertungen
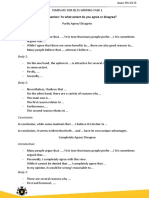
- Question: To What Extent Do You Agree or Disagree?Dokument5 SeitenQuestion: To What Extent Do You Agree or Disagree?tien buiNoch keine Bewertungen
- The PILOT: July 2023Dokument16 SeitenThe PILOT: July 2023RSCA Redwood ShoresNoch keine Bewertungen
- Detroit ManualDokument435 SeitenDetroit Manualvictorhernandezrega50% (2)
- Dominar 400 Spare Parts CatalogueDokument82 SeitenDominar 400 Spare Parts CatalogueAkshayaNoch keine Bewertungen
- Ljubljana European Green Capital 2016Dokument56 SeitenLjubljana European Green Capital 2016Kann_dandy17Noch keine Bewertungen
- Point of View Task CardsDokument7 SeitenPoint of View Task Cardsapi-660227300Noch keine Bewertungen
- Bar Q Salaries Part 2Dokument5 SeitenBar Q Salaries Part 2Brigette DomingoNoch keine Bewertungen
- 1.1 Cruz v. DENR PDFDokument7 Seiten1.1 Cruz v. DENR PDFBenBulacNoch keine Bewertungen
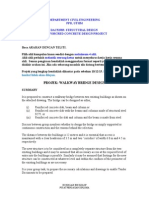
- Projek Rekabentuk Walkwaybridge 2014 - 15Dokument6 SeitenProjek Rekabentuk Walkwaybridge 2014 - 15HambaliNoch keine Bewertungen
- Variable Length Subnet MasksDokument4 SeitenVariable Length Subnet MaskszelalemNoch keine Bewertungen
- Emancipation Fact SheetDokument2 SeitenEmancipation Fact SheetKeelie SmithNoch keine Bewertungen
- Chap 14Dokument31 SeitenChap 14Dipti Bhavin DesaiNoch keine Bewertungen
- The 9 Best Reasons To Choose ZultysDokument13 SeitenThe 9 Best Reasons To Choose ZultysGreg EickeNoch keine Bewertungen
- Nature Hill Middle School Wants To Raise Money For A NewDokument1 SeiteNature Hill Middle School Wants To Raise Money For A NewAmit PandeyNoch keine Bewertungen
- Determination of Sales Force Size - 2Dokument2 SeitenDetermination of Sales Force Size - 2Manish Kumar100% (3)
- Art 3 Sec 2Dokument157 SeitenArt 3 Sec 2KELVINNoch keine Bewertungen
- IMO Publication Catalogue List (June 2022)Dokument17 SeitenIMO Publication Catalogue List (June 2022)Seinn NuNoch keine Bewertungen
- Zone Controller: Th-LargeDokument1 SeiteZone Controller: Th-LargeIsmat AraNoch keine Bewertungen
- MTBE - Module - 3Dokument83 SeitenMTBE - Module - 3ABHIJITH V SNoch keine Bewertungen