Das könnte Ihnen auch gefallen
- Toll Tax ExemptionDokument1 SeiteToll Tax ExemptionShounak Bhattacharyya100% (7)
- Toll Tax ExemptionDokument2 SeitenToll Tax ExemptionVigneshwar Raju Prathikantam100% (1)
- Marathi EpaperDokument9 SeitenMarathi EpapercrimeborderNoch keine Bewertungen
- ServiceBook Format PDFDokument122 SeitenServiceBook Format PDFRajkumar MathurNoch keine Bewertungen
- JUNUKADokument17 SeitenJUNUKAHimjyoti TalukdarNoch keine Bewertungen
- English - AFP Investigation Form - Version - 1st - Dec - 2020Dokument2 SeitenEnglish - AFP Investigation Form - Version - 1st - Dec - 2020Tella AdedamolaNoch keine Bewertungen
- Medical Attendants Certificate17062019Dokument2 SeitenMedical Attendants Certificate17062019PrathameshNoch keine Bewertungen
- PFIZER 5 17 All in 1 FormDokument3 SeitenPFIZER 5 17 All in 1 Formrenz jNoch keine Bewertungen
- Afp Case Investigation FormDokument3 SeitenAfp Case Investigation Formአብይ በላይነሽ ጥላሁንNoch keine Bewertungen
- Form Accident ReportDokument4 SeitenForm Accident ReportKarthik SNoch keine Bewertungen
- Page 1 of 4: PPGNNJ 11/09 Confidential Property of Planned Parenthood of Greater Northern NJ, IncDokument4 SeitenPage 1 of 4: PPGNNJ 11/09 Confidential Property of Planned Parenthood of Greater Northern NJ, IncTINALEETNT723Noch keine Bewertungen
- Lasustech Medical FormDokument2 SeitenLasustech Medical FormAl MubarakNoch keine Bewertungen
- Employee Claim: A. Your Information (Employee)Dokument6 SeitenEmployee Claim: A. Your Information (Employee)dratiffaridNoch keine Bewertungen
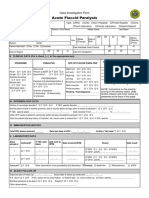
- Case Investigation Form - Acute Flaccid ParalysisDokument2 SeitenCase Investigation Form - Acute Flaccid Paralysisclaverialc10Noch keine Bewertungen
- Medical Form For Grade 7 12Dokument3 SeitenMedical Form For Grade 7 12Deonna Angeline100% (1)
- CT Screening FormDokument1 SeiteCT Screening FormJuliano PachecoNoch keine Bewertungen
- Acute Flaccid Paralysis: Case Investigation FormDokument2 SeitenAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- CDC Data Collection Long FormDokument13 SeitenCDC Data Collection Long FormBanzai Health Private LimitedNoch keine Bewertungen
- Blank Neurodevelopmental Intake FormDokument2 SeitenBlank Neurodevelopmental Intake FormjhecyNoch keine Bewertungen
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDokument3 SeitenViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNoch keine Bewertungen
- TBJ New Patient Registration FormsDokument9 SeitenTBJ New Patient Registration FormsSandra RíosNoch keine Bewertungen
- Appendices: Appendix ADokument27 SeitenAppendices: Appendix AMaria Delia SalvadoNoch keine Bewertungen
- PT Intake FormDokument4 SeitenPT Intake FormChifor FlorinNoch keine Bewertungen
- ReportForm TyphoidDokument2 SeitenReportForm TyphoidSundarajan ManiNoch keine Bewertungen
- Parental Consent Form: To Whom It May ConcernDokument4 SeitenParental Consent Form: To Whom It May ConcernNorman PolilinNoch keine Bewertungen
- CIF-MR 2022 Ver1Dokument2 SeitenCIF-MR 2022 Ver1Ivy marie BonNoch keine Bewertungen
- Postnatal Assessment Tool M.SC NSGDokument12 SeitenPostnatal Assessment Tool M.SC NSGM. jehovah Nissie YeshalomeNoch keine Bewertungen
- Measles CIF 2014Dokument2 SeitenMeasles CIF 2014RionaMarieMagbutayNoch keine Bewertungen
- Graduate PDFDokument2 SeitenGraduate PDFTrieu LeNoch keine Bewertungen
- Cif Zika - 2016 PDFDokument3 SeitenCif Zika - 2016 PDFNicholai CabadduNoch keine Bewertungen
- For Children: Welcome To Our Practice: 4.) Responsible Party Info: 1.) Tell Us About Your ChildDokument2 SeitenFor Children: Welcome To Our Practice: 4.) Responsible Party Info: 1.) Tell Us About Your ChildAnh TranNoch keine Bewertungen
- Common Summary Assessment ReportDokument4 SeitenCommon Summary Assessment ReportVaibhav DafaleNoch keine Bewertungen
- 11 Trauma Emergency Form 19102023Dokument2 Seiten11 Trauma Emergency Form 19102023Marjorie BricenioNoch keine Bewertungen
- Obstetrics History General DataDokument7 SeitenObstetrics History General DataColeen NeyraNoch keine Bewertungen
- CRF HFMD AsmghDokument2 SeitenCRF HFMD AsmghRyeowook RyeNoch keine Bewertungen
- Case Report Form For HFMDDokument2 SeitenCase Report Form For HFMDMendez RhuNoch keine Bewertungen
- Case Investigation Forms - Pidsrmop3ed 1Dokument16 SeitenCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Student Physician FormDokument1 SeiteStudent Physician FormMasr RedaNoch keine Bewertungen
- Annex A. Ambulance Conduction Intial Information SheetDokument2 SeitenAnnex A. Ambulance Conduction Intial Information SheetJoel SantosNoch keine Bewertungen
- Medical Fitness Form PDFDokument4 SeitenMedical Fitness Form PDFKartikeya BagraNoch keine Bewertungen
- Antipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Dokument2 SeitenAntipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Chlong ArtuzNoch keine Bewertungen
- DR Langford1Dokument8 SeitenDR Langford1Spencer JacksonNoch keine Bewertungen
- History TakingDokument6 SeitenHistory Takingdharti daveNoch keine Bewertungen
- Measles Case FormDokument3 SeitenMeasles Case FormVlad BăhneanuNoch keine Bewertungen
- Interview Pa Tool.Dokument5 SeitenInterview Pa Tool.Raisah Bint AbdullahNoch keine Bewertungen
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Dokument21 SeitenAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNoch keine Bewertungen
- Discharge Planning TBDokument2 SeitenDischarge Planning TBNurida LatipahNoch keine Bewertungen
- Surgical Safety ChecklistDokument1 SeiteSurgical Safety ChecklistАндрій ДанильцівNoch keine Bewertungen
- 5 Assesed WoredaDokument59 Seiten5 Assesed WoredaatakltigebertsadikNoch keine Bewertungen
- 7 Unassesed Woreda Copy111Dokument72 Seiten7 Unassesed Woreda Copy111atakltigebertsadikNoch keine Bewertungen
- Gordon S Functional Health Pattern Assessment TooL: EdisonDokument13 SeitenGordon S Functional Health Pattern Assessment TooL: EdisonEdison Olad Dangkeo, RN,RM67% (3)
- Patient Registration Form 29Dokument8 SeitenPatient Registration Form 29Cahayastore CahayastoreNoch keine Bewertungen
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationDokument3 SeitenTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenNoch keine Bewertungen
- Malaria Identification and Counseling FormDokument1 SeiteMalaria Identification and Counseling FormTewodros TafereNoch keine Bewertungen
- Medical Examination Form: Tel Aviv University International International - Tau.Ac - IlDokument6 SeitenMedical Examination Form: Tel Aviv University International International - Tau.Ac - IlSiddaq SinghNoch keine Bewertungen
- Boys State Accident Report Form: InstructionsDokument4 SeitenBoys State Accident Report Form: InstructionsWit worldNoch keine Bewertungen
- Family Health Problem (Common) / Abnormality: (E.g. Uncle)Dokument2 SeitenFamily Health Problem (Common) / Abnormality: (E.g. Uncle)Evelyn Medina100% (1)
- Case Investigation Form - Measles-RubellaDokument2 SeitenCase Investigation Form - Measles-Rubellaclaverialc10Noch keine Bewertungen
- CDC Covid-19 Report FormDokument2 SeitenCDC Covid-19 Report FormiggybauNoch keine Bewertungen
- Barangay Assisted Booking Form: CODE: D1ADokument4 SeitenBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNoch keine Bewertungen
- CJ1W-PRT21 PROFIBUS-DP Slave Unit: Operation ManualDokument100 SeitenCJ1W-PRT21 PROFIBUS-DP Slave Unit: Operation ManualSergio Eu CaNoch keine Bewertungen
- Influence of Brand Experience On CustomerDokument16 SeitenInfluence of Brand Experience On Customerarif adrianNoch keine Bewertungen
- Indian RailwaysDokument20 SeitenIndian RailwaysNirmalNoch keine Bewertungen
- Financial Management Full Notes at Mba FinanceDokument44 SeitenFinancial Management Full Notes at Mba FinanceBabasab Patil (Karrisatte)86% (7)
- Wall Chart - Drying - How Wood Loses MoistureDokument1 SeiteWall Chart - Drying - How Wood Loses MoistureXihuitl61100% (1)
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Dokument3 SeitenHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniNoch keine Bewertungen
- (NewResultBD - Com) Mymensingh Board JSC Scholarship Result 2019Dokument80 Seiten(NewResultBD - Com) Mymensingh Board JSC Scholarship Result 2019rthedthbdeth100% (1)
- Jaringan Noordin M. TopDokument38 SeitenJaringan Noordin M. TopgiantoNoch keine Bewertungen
- Kanne Gerber Et Al Vineland 2010Dokument12 SeitenKanne Gerber Et Al Vineland 2010Gh8jfyjnNoch keine Bewertungen
- 9701 w19 QP 21 PDFDokument12 Seiten9701 w19 QP 21 PDFFaiza KhalidNoch keine Bewertungen
- 659.69 BM67 2018-02-06 02 Im Beu-UsaDokument88 Seiten659.69 BM67 2018-02-06 02 Im Beu-UsaIrakli JibladzeNoch keine Bewertungen
- Chem HazardsDokument17 SeitenChem HazardsMJ NuarinNoch keine Bewertungen
- Soal CautionDokument10 SeitenSoal Cautionadhyatnika geusan ulun50% (2)
- Investment ChecklistDokument3 SeitenInvestment ChecklistArpan chakrabortyNoch keine Bewertungen
- Italian Companies Eastern China - JAN 2014Dokument139 SeitenItalian Companies Eastern China - JAN 2014AndresNoch keine Bewertungen
- TLE10 - Q3 - Lesson 5Dokument17 SeitenTLE10 - Q3 - Lesson 5Ella Cagadas PuzonNoch keine Bewertungen
- TEMPLATE Keputusan Peperiksaan THP 1Dokument49 SeitenTEMPLATE Keputusan Peperiksaan THP 1SABERI BIN BANDU KPM-GuruNoch keine Bewertungen
- Oracle Database 12c r2 Administration Workshop Ed 3Dokument7 SeitenOracle Database 12c r2 Administration Workshop Ed 3Firas ChaabeneNoch keine Bewertungen
- George Herbert Scherff Walker Bush: Agentur of The New World OrderDokument36 SeitenGeorge Herbert Scherff Walker Bush: Agentur of The New World Orderextemporaneous100% (3)
- Quantum PauseDokument5 SeitenQuantum Pausesoulsearch67641100% (2)
- GO 44 RUDA ExpansionDokument4 SeitenGO 44 RUDA ExpansionbharathNoch keine Bewertungen
- MinimumEHS Standards For Projects-V3Dokument113 SeitenMinimumEHS Standards For Projects-V3Ammu KuttiyNoch keine Bewertungen
- MAELLT Brochure 2006-1Dokument2 SeitenMAELLT Brochure 2006-1Ryan Glenn Cedan CondaNoch keine Bewertungen
- D245S 734046 Om enDokument90 SeitenD245S 734046 Om enEndro Accoustic100% (1)
- 2019 - List of Equipment, Tools & MaterialsDokument3 Seiten2019 - List of Equipment, Tools & Materialsreynald manzanoNoch keine Bewertungen
- AS Unit 1 Revision Note Physics IAL EdexcelDokument9 SeitenAS Unit 1 Revision Note Physics IAL EdexcelMahbub Khan100% (1)
- Fujiwheel CatalogDokument16 SeitenFujiwheel CatalogKhaeri El BarbasyNoch keine Bewertungen
- PSCI101 - Prelims ReviewerDokument3 SeitenPSCI101 - Prelims RevieweremmanuelcambaNoch keine Bewertungen
- Product Bulletin Fisher 8580 Rotary Valve en 123032Dokument16 SeitenProduct Bulletin Fisher 8580 Rotary Valve en 123032Rachmat MaulanaNoch keine Bewertungen
- Metsec Steel Framing SystemDokument46 SeitenMetsec Steel Framing Systemleonil7Noch keine Bewertungen