Das könnte Ihnen auch gefallen
- Feb-19 Feb-19 Feb-19 Feb-19 Feb-19 Feb-19 Feb-19 Feb-19Dokument5 SeitenFeb-19 Feb-19 Feb-19 Feb-19 Feb-19 Feb-19 Feb-19 Feb-19Desmiyati AdoeNoch keine Bewertungen
- Original Contributions: A Randomized Trial Comparing Metered Dose Inhalers and Breath Actuated NebulizersDokument8 SeitenOriginal Contributions: A Randomized Trial Comparing Metered Dose Inhalers and Breath Actuated NebulizersDesmiyati AdoeNoch keine Bewertungen
- Assessment of Clinical Outcome of Children With Sepsis Outside The Intensive Care UnitDokument9 SeitenAssessment of Clinical Outcome of Children With Sepsis Outside The Intensive Care UnitDesmiyati AdoeNoch keine Bewertungen
- Can Tey 2018Dokument6 SeitenCan Tey 2018Desmiyati AdoeNoch keine Bewertungen
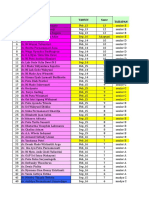
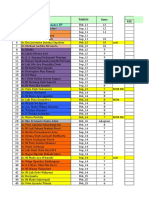
- No Nama Tahun SMTR TahapanDokument15 SeitenNo Nama Tahun SMTR TahapanDesmiyati AdoeNoch keine Bewertungen
- Shankaran 2019Dokument11 SeitenShankaran 2019Desmiyati AdoeNoch keine Bewertungen
- Jurnal NeonatusDokument41 SeitenJurnal NeonatusDesmiyati AdoeNoch keine Bewertungen
- Glasgow Coma Scale For Infants Children PDFDokument1 SeiteGlasgow Coma Scale For Infants Children PDFDesmiyati AdoeNoch keine Bewertungen
- 11 Rotasi Nop-18Dokument5 Seiten11 Rotasi Nop-18Desmiyati AdoeNoch keine Bewertungen
- Bilirubin Less Than 35 WeeksDokument8 SeitenBilirubin Less Than 35 WeeksDesmiyati AdoeNoch keine Bewertungen
- Rotasi PpdsDokument13 SeitenRotasi PpdsDesmiyati AdoeNoch keine Bewertungen
- NO Program Program Book Scientific Program FileDokument2 SeitenNO Program Program Book Scientific Program FileDesmiyati AdoeNoch keine Bewertungen
- Leaflet ACTIA MULLER Garage EquipmentDokument52 SeitenLeaflet ACTIA MULLER Garage Equipmentnicolas_perrierNoch keine Bewertungen
- Neonatal Guidelines PDF 2015-17 With Links PDFDokument364 SeitenNeonatal Guidelines PDF 2015-17 With Links PDFJhonny Marquez100% (11)
- Dr. Ni Luh Putu Surya Candra EP: No Nama Tahun SMTR Jan - 18Dokument90 SeitenDr. Ni Luh Putu Surya Candra EP: No Nama Tahun SMTR Jan - 18Desmiyati AdoeNoch keine Bewertungen
- 5 6057344157398073400Dokument69 Seiten5 6057344157398073400Desmiyati AdoeNoch keine Bewertungen
- No Nama Februari 2018: Jadwal Jaga Residen Ika FK Unud/Rsup Sanglah Bulan Februari 2018Dokument4 SeitenNo Nama Februari 2018: Jadwal Jaga Residen Ika FK Unud/Rsup Sanglah Bulan Februari 2018Desmiyati AdoeNoch keine Bewertungen
- Form Kosong PneumoniaDokument6 SeitenForm Kosong PneumoniaDesmiyati AdoeNoch keine Bewertungen
- Laporan Jaga Sabtu Malam, 10 Februari 2018Dokument14 SeitenLaporan Jaga Sabtu Malam, 10 Februari 2018Desmiyati AdoeNoch keine Bewertungen
- New Doc 2018-03-23 - 17Dokument1 SeiteNew Doc 2018-03-23 - 17Desmiyati AdoeNoch keine Bewertungen
- Antimicrobial Stewardship ProgrammeDokument12 SeitenAntimicrobial Stewardship ProgrammeDesmiyati AdoeNoch keine Bewertungen
- NO Nama Dokter Indeks Jasa MedisDokument2 SeitenNO Nama Dokter Indeks Jasa MedisDesmiyati AdoeNoch keine Bewertungen
- BagianA PDFDokument68 SeitenBagianA PDFDesmiyati AdoeNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Advanced Techniques in Diagnostic MicrobiologyDokument14 SeitenAdvanced Techniques in Diagnostic MicrobiologyTumabang DivineNoch keine Bewertungen
- 2013 Book EpigeneticsDevelopmentAndDisea PDFDokument698 Seiten2013 Book EpigeneticsDevelopmentAndDisea PDFSuelen Lima de Matos100% (1)
- Important Notice: List of Life Members of AMI Enrolled Upto 31.3.2010Dokument137 SeitenImportant Notice: List of Life Members of AMI Enrolled Upto 31.3.2010avinashdeo0% (1)
- 18 ACVVR FinalDokument58 Seiten18 ACVVR FinalElison J PanggaloNoch keine Bewertungen
- VONRESORT Golden Beach, Side: DescriereDokument2 SeitenVONRESORT Golden Beach, Side: DescriereCorina ZuleanuNoch keine Bewertungen
- Lecture 1 Introduction To Virology 213-CLSM L4Dokument17 SeitenLecture 1 Introduction To Virology 213-CLSM L4Fwaaz AlbarqiNoch keine Bewertungen
- Hepatitis B: The Immaculate Infection: Annmarie Huysman, MD Mitul Patel, MD Douglas T. Dieterich, MDDokument7 SeitenHepatitis B: The Immaculate Infection: Annmarie Huysman, MD Mitul Patel, MD Douglas T. Dieterich, MDEnwunlu Bosso ThomasNoch keine Bewertungen
- Non Mendelian LEDokument7 SeitenNon Mendelian LECRESELDA VANGUARDIANoch keine Bewertungen
- Microbiology NotesDokument3 SeitenMicrobiology NotesAthena Huynh100% (1)
- Structure of Gene and Types of MutationDokument68 SeitenStructure of Gene and Types of Mutationnavashreeraji3986Noch keine Bewertungen
- Metagenomics and Industrial Applications: PerspectivesDokument7 SeitenMetagenomics and Industrial Applications: PerspectivesMariaNoch keine Bewertungen
- DNA and PROTEIN SYNTHESIS MODULE OVERVIEW 2012Dokument29 SeitenDNA and PROTEIN SYNTHESIS MODULE OVERVIEW 2012Desiree CastilloNoch keine Bewertungen
- Happy Birthday PaperDokument1 SeiteHappy Birthday PaperSahil LakhaniNoch keine Bewertungen
- CSR SaladDokument16 SeitenCSR SaladDaniel Caballero CerbonNoch keine Bewertungen
- Probiotics GuidelinesDokument20 SeitenProbiotics GuidelinesMadan Mohan Sharan SinghNoch keine Bewertungen
- GENETICSDokument196 SeitenGENETICSJulianne PetargueNoch keine Bewertungen
- Medical Student Elective Book Spring 2020: Updated 08/13/2020Dokument234 SeitenMedical Student Elective Book Spring 2020: Updated 08/13/2020ayeshaNoch keine Bewertungen
- Intro To LifeDokument32 SeitenIntro To LifeMaricar Paz100% (1)
- CHAPTER III-3. The Cellular Basis of Life: Self TestDokument8 SeitenCHAPTER III-3. The Cellular Basis of Life: Self TestLyka Abdullah TayuanNoch keine Bewertungen
- Sci9 - Q1 - M3 - Location of Genes in Chromosomes - V5Dokument21 SeitenSci9 - Q1 - M3 - Location of Genes in Chromosomes - V5Ceejay Concon75% (4)
- Pharma Domain 101 - The Industry Lingo (Latest)Dokument10 SeitenPharma Domain 101 - The Industry Lingo (Latest)Ankit AgarwalNoch keine Bewertungen
- Drug Development Process Cleveland, 6.23.06Dokument65 SeitenDrug Development Process Cleveland, 6.23.06Srinivasa Chary SriramadasuNoch keine Bewertungen
- Parts of A CellDokument4 SeitenParts of A CelltadashiiNoch keine Bewertungen
- Exercise 1 Gametogenesis ReviewerDokument4 SeitenExercise 1 Gametogenesis ReviewerJasper AdonisNoch keine Bewertungen
- Agrobacterium Tumefaciens:: Scientific ClassificationDokument3 SeitenAgrobacterium Tumefaciens:: Scientific ClassificationMuhammad Amjad AkhlasNoch keine Bewertungen
- Kapoy Buhat HiihhhhDokument15 SeitenKapoy Buhat Hiihhhhramil_sanchezNoch keine Bewertungen
- Pengetahuan, Sikap Dan Etika Batuk Pada Penderita Tuberkulosis ParuDokument8 SeitenPengetahuan, Sikap Dan Etika Batuk Pada Penderita Tuberkulosis ParuNurafni LativamcbNoch keine Bewertungen
- Teacher Guide, HS Biology - Genetic VariationDokument13 SeitenTeacher Guide, HS Biology - Genetic VariationGlaine GemperoaNoch keine Bewertungen
- Bacterial TransformationDokument18 SeitenBacterial TransformationBhawna Gautam100% (1)
- Wolfgang R. Streit, Rolf Daniel Eds. Metagenomics Methods and ProtocolsDokument311 SeitenWolfgang R. Streit, Rolf Daniel Eds. Metagenomics Methods and ProtocolsEmmanuel UrbinaNoch keine Bewertungen