Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Moses Mabhida Stadium PDFDokument4 SeitenMoses Mabhida Stadium PDFHCStepNoch keine Bewertungen
- Grade 4 Decimals: Answer The QuestionsDokument4 SeitenGrade 4 Decimals: Answer The QuestionsEduGainNoch keine Bewertungen
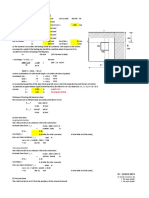
- Iso With Eccentric LoadingDokument12 SeitenIso With Eccentric Loadingsaubhagya majhiNoch keine Bewertungen
- Grade 8 Math W2 LASDokument19 SeitenGrade 8 Math W2 LASJaeda BaltazarNoch keine Bewertungen
- K.T. Chau, R.H.C. Wong, T.-f. Wong (Auth.), STAVROS K. KOURKOULIS (Eds.) - Fracture and Failure of Natural Building Stones_ Applications in the Restoration of Ancient Monuments-Springer Netherlands (2Dokument581 SeitenK.T. Chau, R.H.C. Wong, T.-f. Wong (Auth.), STAVROS K. KOURKOULIS (Eds.) - Fracture and Failure of Natural Building Stones_ Applications in the Restoration of Ancient Monuments-Springer Netherlands (2Daniel Ruperto CanoNoch keine Bewertungen
- Comparison of Efficacy and Safety of Intracervical Foleys Catheter Balloon With Intracervical Prostaglandin E2 Gel (Dinoprostone) For Induction of Labour.Dokument9 SeitenComparison of Efficacy and Safety of Intracervical Foleys Catheter Balloon With Intracervical Prostaglandin E2 Gel (Dinoprostone) For Induction of Labour.Anonymous HXZigeNoch keine Bewertungen
- Effect of Operational Goals and Objectives On Implementation of Nhis in Ghana and Nigeria.Dokument6 SeitenEffect of Operational Goals and Objectives On Implementation of Nhis in Ghana and Nigeria.Anonymous HXZigeNoch keine Bewertungen
- Prebiotics and Probiotics in Ayurveda.Dokument4 SeitenPrebiotics and Probiotics in Ayurveda.Anonymous HXZigeNoch keine Bewertungen
- The Association and Differences of Overuse Injury Occurrences and Training Related Supportive Factors in Ethiopian Youth Running Athletes.Dokument9 SeitenThe Association and Differences of Overuse Injury Occurrences and Training Related Supportive Factors in Ethiopian Youth Running Athletes.Anonymous HXZigeNoch keine Bewertungen
- Evaluation of Root and Canal Morphology of Maxillary Permanent Premolars in An Egyptian Population by Cone-Beam Computed Tomography.Dokument7 SeitenEvaluation of Root and Canal Morphology of Maxillary Permanent Premolars in An Egyptian Population by Cone-Beam Computed Tomography.Anonymous HXZigeNoch keine Bewertungen
- An Hepatic Nodule Not Like The Others.Dokument2 SeitenAn Hepatic Nodule Not Like The Others.Anonymous HXZigeNoch keine Bewertungen
- Maternal and Perinatal Outcome in Pregnancies Complicated With Hypertensive Disorder of Pregnancy.Dokument8 SeitenMaternal and Perinatal Outcome in Pregnancies Complicated With Hypertensive Disorder of Pregnancy.Anonymous HXZigeNoch keine Bewertungen
- A Study On Job Satisfaction With Reference To Transport Employees in Kumbakonam Region, Tamilnadu.Dokument5 SeitenA Study On Job Satisfaction With Reference To Transport Employees in Kumbakonam Region, Tamilnadu.Anonymous HXZigeNoch keine Bewertungen
- Comparison of Balance Between The Normal Vision & Visually Impaired School Children Using The Balance Evaluation Systems Test (Bestest) .Dokument8 SeitenComparison of Balance Between The Normal Vision & Visually Impaired School Children Using The Balance Evaluation Systems Test (Bestest) .Anonymous HXZigeNoch keine Bewertungen
- Late-Presenting Bochdalek Hernia: A Rare Cause of Acute Abdominal Pain in Adults.Dokument3 SeitenLate-Presenting Bochdalek Hernia: A Rare Cause of Acute Abdominal Pain in Adults.Anonymous HXZigeNoch keine Bewertungen
- Molecular Spectroscopy Characterization of Binary Liquid Mixtures Using Attenuated Total Reflectance-Fourier Transforms Infrared Approach.Dokument6 SeitenMolecular Spectroscopy Characterization of Binary Liquid Mixtures Using Attenuated Total Reflectance-Fourier Transforms Infrared Approach.Anonymous HXZigeNoch keine Bewertungen
- The Contribution of Geographic Information Systems and Remote Sensing in Urban Management: Case of Urban Agencies in Morocco.Dokument7 SeitenThe Contribution of Geographic Information Systems and Remote Sensing in Urban Management: Case of Urban Agencies in Morocco.Anonymous HXZigeNoch keine Bewertungen
- Journal Homepage: - : IntroductionDokument11 SeitenJournal Homepage: - : IntroductionAnonymous HXZigeNoch keine Bewertungen
- Effect of Operational Goals and Objectives On Implementation of Nhis in Ghana and Nigeria.Dokument6 SeitenEffect of Operational Goals and Objectives On Implementation of Nhis in Ghana and Nigeria.Anonymous HXZigeNoch keine Bewertungen
- Professional Learning Communities in Relation To Teachers Efficacy and Students Achievement.Dokument8 SeitenProfessional Learning Communities in Relation To Teachers Efficacy and Students Achievement.Anonymous HXZigeNoch keine Bewertungen
- Solid Waste Management in Tamil Nadu.Dokument4 SeitenSolid Waste Management in Tamil Nadu.Anonymous HXZige100% (1)
- A Study On Consumer Perception Towards Nandini Dairy Products in Chamarajanagar District of Karnataka.Dokument8 SeitenA Study On Consumer Perception Towards Nandini Dairy Products in Chamarajanagar District of Karnataka.Anonymous HXZigeNoch keine Bewertungen
- Journal Homepage: - : IntroductionDokument12 SeitenJournal Homepage: - : IntroductionAnonymous HXZigeNoch keine Bewertungen
- Journal Homepage: - : IntroductionDokument10 SeitenJournal Homepage: - : IntroductionAnonymous HXZigeNoch keine Bewertungen
- Controlling The Pollution of Surabaya River Based On The Study of Ipal (Ijin Pembuangan Air Limbah) Conduct.Dokument7 SeitenControlling The Pollution of Surabaya River Based On The Study of Ipal (Ijin Pembuangan Air Limbah) Conduct.Anonymous HXZigeNoch keine Bewertungen
- Journal Homepage: - : Manuscript HistoryDokument7 SeitenJournal Homepage: - : Manuscript HistoryAnonymous HXZigeNoch keine Bewertungen
- Thyroid Disorders Among Patients Visiting Tertiary Health Care Centre in Eastern Uttar Pradesh.Dokument5 SeitenThyroid Disorders Among Patients Visiting Tertiary Health Care Centre in Eastern Uttar Pradesh.Anonymous HXZigeNoch keine Bewertungen
- Reliability of Shadow Goniometer For Thoracolumbar Spine Extension Range of Motion.Dokument5 SeitenReliability of Shadow Goniometer For Thoracolumbar Spine Extension Range of Motion.Anonymous HXZigeNoch keine Bewertungen
- COMPARATIVE STUDY TO ASSESS THE EFFECTIVENESS OF OBJECTIVE STRUCTURED CLINICAL EXAMINATION (OSCE) VERSES TRADITIONAL METHOD IN TERMS OF KNOWLEDGE REGARDING ANTENATAL EXAMINATION AMONG B.SC. NURSING 3RD YEAR STUDENTS.Dokument4 SeitenCOMPARATIVE STUDY TO ASSESS THE EFFECTIVENESS OF OBJECTIVE STRUCTURED CLINICAL EXAMINATION (OSCE) VERSES TRADITIONAL METHOD IN TERMS OF KNOWLEDGE REGARDING ANTENATAL EXAMINATION AMONG B.SC. NURSING 3RD YEAR STUDENTS.Anonymous HXZigeNoch keine Bewertungen
- The Treatment of Traumatic Brain Injury in Experimental Animals by Pyrimidine Derivatives.Dokument5 SeitenThe Treatment of Traumatic Brain Injury in Experimental Animals by Pyrimidine Derivatives.Anonymous HXZigeNoch keine Bewertungen
- Influence of Educational Program On Social Maturity Among Children Residing in Orphanages.Dokument9 SeitenInfluence of Educational Program On Social Maturity Among Children Residing in Orphanages.Anonymous HXZigeNoch keine Bewertungen
- An Emperical Study of Demonetization & Its Impact On Rethinking of Tax Disclosure - A Study Based On National Capital Region.Dokument11 SeitenAn Emperical Study of Demonetization & Its Impact On Rethinking of Tax Disclosure - A Study Based On National Capital Region.Anonymous HXZigeNoch keine Bewertungen
- Journal Homepage: - : Associate Professor, Dentistry Program,, Assistant Professor, Dentistry ProgramDokument10 SeitenJournal Homepage: - : Associate Professor, Dentistry Program,, Assistant Professor, Dentistry ProgramAnonymous HXZigeNoch keine Bewertungen
- Knowledge, Attitude, and Practice Regarding Evidence Based Dentistry Among Dentists of Hazaribag, Jharkhand, India.Dokument7 SeitenKnowledge, Attitude, and Practice Regarding Evidence Based Dentistry Among Dentists of Hazaribag, Jharkhand, India.Anonymous HXZigeNoch keine Bewertungen
- A Study of Attachment Style Among Learning Disabled Childrenin Comparison To Non Learning Disabled Children.Dokument3 SeitenA Study of Attachment Style Among Learning Disabled Childrenin Comparison To Non Learning Disabled Children.Anonymous HXZige100% (1)
- MWM Parts ListDokument6 SeitenMWM Parts ListRuy PeñaNoch keine Bewertungen
- Management - Ch06 - Forecasting and PremisingDokument9 SeitenManagement - Ch06 - Forecasting and PremisingRameshKumarMurali0% (1)
- Chapter 2 P2 Section ADokument27 SeitenChapter 2 P2 Section ANurul 'AinNoch keine Bewertungen
- Important Notes of 10th Class Math Exercise 3.2Dokument12 SeitenImportant Notes of 10th Class Math Exercise 3.2Tayyabah ShahNoch keine Bewertungen
- Triple Chocolate Layer Cake Triple Chocolate Layer CakeDokument3 SeitenTriple Chocolate Layer Cake Triple Chocolate Layer CakeJuhyun LeeNoch keine Bewertungen
- PROG 8011 Lab 6-W24Dokument2 SeitenPROG 8011 Lab 6-W24kaurrrjass1125Noch keine Bewertungen
- ReviewerDokument6 SeitenReviewerNeo GarceraNoch keine Bewertungen
- Person Name: NDT Management CoordinatorDokument4 SeitenPerson Name: NDT Management CoordinatorDendy PratamaNoch keine Bewertungen
- Solar Radiation, Heat Balance and Temperature Chapter 8 - Class 11 Geography NCERT - Class Notes - Samagra Book Series Batch (Hinglish)Dokument30 SeitenSolar Radiation, Heat Balance and Temperature Chapter 8 - Class 11 Geography NCERT - Class Notes - Samagra Book Series Batch (Hinglish)avnish.k.verma.2014Noch keine Bewertungen
- MAT3700-MayJune ExamDokument3 SeitenMAT3700-MayJune ExamNhlanhla NdebeleNoch keine Bewertungen
- ELTE 307 - DR Mohamed Sobh-Lec - 5-1-11-2022Dokument28 SeitenELTE 307 - DR Mohamed Sobh-Lec - 5-1-11-2022Lina ElsayedNoch keine Bewertungen
- Opsis Technique Eng 2007Dokument4 SeitenOpsis Technique Eng 2007sukumariicbNoch keine Bewertungen
- Production ManagementDokument14 SeitenProduction Managementavinasss1963_3707255Noch keine Bewertungen
- Robotics 1 - Coordinate SystemDokument102 SeitenRobotics 1 - Coordinate System15.Rushikesh IrabattinNoch keine Bewertungen
- Alpha ParticleDokument12 SeitenAlpha ParticlechristineNoch keine Bewertungen
- 2022 Cayley Contest: The Centre For Education in Mathematics and Computing Cemc - Uwaterloo.caDokument282 Seiten2022 Cayley Contest: The Centre For Education in Mathematics and Computing Cemc - Uwaterloo.catony dooNoch keine Bewertungen
- CAPTAIN250DITEINCOMPLETEAug 2020Dokument15 SeitenCAPTAIN250DITEINCOMPLETEAug 2020billal toufik BendjimaNoch keine Bewertungen
- Av02 2516enDokument13 SeitenAv02 2516enpagol_23_smhNoch keine Bewertungen
- K-D Hawk: Manitou North America, IncDokument334 SeitenK-D Hawk: Manitou North America, IncRazvan MitruNoch keine Bewertungen
- 4.2 Programming - BottomUpWorkflow (OneStripe) - Exercise06Dokument11 Seiten4.2 Programming - BottomUpWorkflow (OneStripe) - Exercise06fernandoNoch keine Bewertungen
- Series: 973 - 1327 KWM (Gross) at 1500 RPMDokument18 SeitenSeries: 973 - 1327 KWM (Gross) at 1500 RPMlahcen boudaoudNoch keine Bewertungen
- BP301T Poc Unit IiiDokument15 SeitenBP301T Poc Unit IiiSUBHASISH DASHNoch keine Bewertungen
- LN 10.5 Ttdomug En-UsDokument82 SeitenLN 10.5 Ttdomug En-UstomactinNoch keine Bewertungen
- 3 Types of Emergency Shutdown and Emergency Isolation ValvesDokument4 Seiten3 Types of Emergency Shutdown and Emergency Isolation ValvesMateusz KonopnickiNoch keine Bewertungen
- Pay It ForwardDokument4 SeitenPay It ForwardAndrew FarrellNoch keine Bewertungen