Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- TctmanualDokument119 SeitenTctmanualAzzaya DashzevegNoch keine Bewertungen
- Ebook PDF Understanding Human Resources Management A Canadian Perspective PDFDokument41 SeitenEbook PDF Understanding Human Resources Management A Canadian Perspective PDFferne.bass217100% (34)
- Salient Points Regarding Changes in PG 2021.Dokument2 SeitenSalient Points Regarding Changes in PG 2021.Srikar BharadwajNoch keine Bewertungen
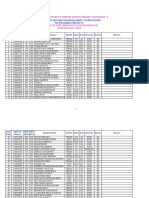
- Final PG Medical Merit List 2021Dokument130 SeitenFinal PG Medical Merit List 2021Srikar BharadwajNoch keine Bewertungen
- MQ Notification For Online 2021-22Dokument6 SeitenMQ Notification For Online 2021-22Srikar BharadwajNoch keine Bewertungen
- Andhra Pradesh Allotments Phase 1 2020Dokument28 SeitenAndhra Pradesh Allotments Phase 1 2020Srikar BharadwajNoch keine Bewertungen
- PG Medical CQ Prospecuts 202Dokument50 SeitenPG Medical CQ Prospecuts 202Srikar BharadwajNoch keine Bewertungen
- Round 2 Total Seats For PG 2021 CounsellingDokument600 SeitenRound 2 Total Seats For PG 2021 CounsellingSrikar BharadwajNoch keine Bewertungen
- Closing Ranks R1 2019 AIQ OnlyDokument2 SeitenClosing Ranks R1 2019 AIQ OnlySrikar BharadwajNoch keine Bewertungen
- Beet PG 2019Dokument104 SeitenBeet PG 2019Srikar BharadwajNoch keine Bewertungen
- Dream School Worksheet PDFDokument2 SeitenDream School Worksheet PDFPaula Cristina Mondaca AlfaroNoch keine Bewertungen
- This Article Is About Organization and CoordinationDokument9 SeitenThis Article Is About Organization and Coordinationakhilesh222Noch keine Bewertungen
- 8607Dokument45 Seiten8607Emaan50% (2)
- Fahrenheit 451 Web QuestDokument5 SeitenFahrenheit 451 Web Questapi-306538760Noch keine Bewertungen
- Doing Business in SeoulDokument38 SeitenDoing Business in SeoulJust BasumataryNoch keine Bewertungen
- English File: Answer SheetDokument1 SeiteEnglish File: Answer SheetMonika aqwerNoch keine Bewertungen
- Chapter One 1.1 Background of The StudyDokument28 SeitenChapter One 1.1 Background of The StudySolace AdeyemiNoch keine Bewertungen
- Rizwan Sajid 2 Page CVDokument2 SeitenRizwan Sajid 2 Page CVRizwanNoch keine Bewertungen
- Training Assessment Report by USAID 4 NigeriaDokument50 SeitenTraining Assessment Report by USAID 4 NigeriaDanial2296Noch keine Bewertungen
- Sample WHLPDokument5 SeitenSample WHLPJumelyn De Luna PalaganasNoch keine Bewertungen
- WWW - Srimed.ro: 4-5 June 2014Dokument2 SeitenWWW - Srimed.ro: 4-5 June 2014David RiveraNoch keine Bewertungen
- Sabour Agri JobDokument8 SeitenSabour Agri JobBipul BiplavNoch keine Bewertungen
- Assignment 1 Lesson Plan RationaleDokument33 SeitenAssignment 1 Lesson Plan Rationaleapi-320967641Noch keine Bewertungen
- Notre Dame of Dadiangas University Notre Dame of Kidapawan CollegeDokument16 SeitenNotre Dame of Dadiangas University Notre Dame of Kidapawan CollegeJames Domini Lopez LabianoNoch keine Bewertungen
- Eenadu - Current Job OpeningsDokument1 SeiteEenadu - Current Job OpeningskasyapNoch keine Bewertungen
- Enhancing The Reading Ability Level of Grade 1 Learners Using Downloaded, Printed Reading MaterialsDokument37 SeitenEnhancing The Reading Ability Level of Grade 1 Learners Using Downloaded, Printed Reading MaterialsJANICE ANGGOTNoch keine Bewertungen
- Gagné (1984)Dokument1 SeiteGagné (1984)IgnacioNoch keine Bewertungen
- Assignment 1 ,,, Significance of ESDDokument7 SeitenAssignment 1 ,,, Significance of ESDNayab Amjad Nayab AmjadNoch keine Bewertungen
- Aqa A Level Gde Bound Jan11Dokument10 SeitenAqa A Level Gde Bound Jan11Diane GrayNoch keine Bewertungen
- Mini Pupillage Cover LetterDokument7 SeitenMini Pupillage Cover Letterfspvwrzh100% (1)
- Dear Student 2013Dokument1 SeiteDear Student 2013Popescu RoxanaNoch keine Bewertungen
- Procedure For Doing Project Work in IIT BombayDokument1 SeiteProcedure For Doing Project Work in IIT BombaySouba GiridharNoch keine Bewertungen
- Khaleb Straight - The Byzantine Empire Russia and Eastern Europe Unit - FinalDokument170 SeitenKhaleb Straight - The Byzantine Empire Russia and Eastern Europe Unit - Finalapi-269480354100% (1)
- The Concept of Vakrokti in Sanskrit PoeticsDokument217 SeitenThe Concept of Vakrokti in Sanskrit Poeticssiva.radha100% (1)
- The Conqueror of Hearts by Shaykh Mustafa Kamal NaqshbandiDokument103 SeitenThe Conqueror of Hearts by Shaykh Mustafa Kamal NaqshbandiAbdul Mateen100% (1)
- California Budget Summary 2018-19Dokument272 SeitenCalifornia Budget Summary 2018-19Capital Public Radio100% (1)
- Method of Wage DeterminationDokument3 SeitenMethod of Wage DeterminationPoonam SatapathyNoch keine Bewertungen
- PowerPoint Slides To PCS Chapter 01 Part BDokument22 SeitenPowerPoint Slides To PCS Chapter 01 Part BSudhanshu VermaNoch keine Bewertungen