Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Whole Sign HousesDokument45 SeitenWhole Sign HousesPhito Perrot88% (8)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Store - Deekeimixes 5 Pro-Tips To MasteringDokument7 SeitenStore - Deekeimixes 5 Pro-Tips To MasteringMalik ANoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Rubber Eggs PDFDokument13 SeitenRubber Eggs PDFShubh dinNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Mix Prep GuideDokument4 SeitenMix Prep GuideMalik A100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- 5 Types of Compressors and When To Use Them: by @deekeimixesDokument6 Seiten5 Types of Compressors and When To Use Them: by @deekeimixesMalik ANoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
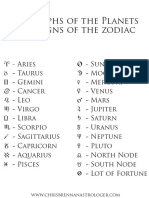
- Astrological GlyphsDokument1 SeiteAstrological GlyphsMalik ANoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- JU-06 Sound List E01 WDokument1 SeiteJU-06 Sound List E01 WGonzalo DelfinoNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- ANZCOR Guideline 2 - Managing An Emergency: Who Does This Guideline Apply To?Dokument4 SeitenANZCOR Guideline 2 - Managing An Emergency: Who Does This Guideline Apply To?Malik ANoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Orestes and Gregorian Mass - ScoresDokument11 SeitenOrestes and Gregorian Mass - ScoresMalik ANoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Owner's Manual For The Human Body: "A Guide To Natural Health, Healing and Longevity"Dokument124 SeitenOwner's Manual For The Human Body: "A Guide To Natural Health, Healing and Longevity"sanjay singh100% (1)
- Warm Up Exercises TipsDokument1 SeiteWarm Up Exercises TipsMalik ANoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Composer List FinalsDokument2 SeitenComposer List FinalsMalik ANoch keine Bewertungen
- Spirit Break Out-G PDFDokument1 SeiteSpirit Break Out-G PDFMalik ANoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- UsbFix ReportDokument5 SeitenUsbFix ReportMalik ANoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Underground Wellness Radio #337: Hacking Your Heart Health With Dr. Joel KahnDokument1 SeiteUnderground Wellness Radio #337: Hacking Your Heart Health With Dr. Joel KahnMalik ANoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- 10 Steps To Earning Awesome GradesDokument88 Seiten10 Steps To Earning Awesome GradesKamal100% (7)
- Healthiest Beans PDFDokument7 SeitenHealthiest Beans PDFMalik ANoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Your HEXACO-PI-R Results: Warning: Your Results Are Very Likely Invalid Due To Inattentive RespondingDokument6 SeitenYour HEXACO-PI-R Results: Warning: Your Results Are Very Likely Invalid Due To Inattentive RespondingMichael John BegalmeNoch keine Bewertungen
- Pluralsight Ultimate Guide Developer PDFDokument8 SeitenPluralsight Ultimate Guide Developer PDFJoe MarshallNoch keine Bewertungen
- The Prefrontal Cortex Anatomy, Physiology and Neuropsychology of The Frontal LobeDokument2 SeitenThe Prefrontal Cortex Anatomy, Physiology and Neuropsychology of The Frontal LobeMalik ANoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 337 Joel KahnDokument19 Seiten337 Joel KahnMalik ANoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Verschaeveetal. RadiatRes 2006 165 598-607Dokument11 SeitenVerschaeveetal. RadiatRes 2006 165 598-607Malik ANoch keine Bewertungen
- Verschaeveetal. RadiatRes 2006 165 598-607 PDFDokument11 SeitenVerschaeveetal. RadiatRes 2006 165 598-607 PDFMalik ANoch keine Bewertungen
- High Fi Delity: Hearing ProtectionDokument2 SeitenHigh Fi Delity: Hearing ProtectionMalik ANoch keine Bewertungen
- Linear Meter Conversion ChartDokument1 SeiteLinear Meter Conversion ChartMalik ANoch keine Bewertungen
- Lord, Keep Me Day by Day - Lyrics PDFDokument1 SeiteLord, Keep Me Day by Day - Lyrics PDFMalik ANoch keine Bewertungen
- Healthiest Beans PDFDokument7 SeitenHealthiest Beans PDFMalik ANoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Lord, Keep Me Day by Day - Lyrics PDFDokument1 SeiteLord, Keep Me Day by Day - Lyrics PDFMalik ANoch keine Bewertungen
- Pluralsight Ultimate Guide Developer PDFDokument8 SeitenPluralsight Ultimate Guide Developer PDFJoe MarshallNoch keine Bewertungen
- Healthiest Beans by Nutrient Density ScoreDokument7 SeitenHealthiest Beans by Nutrient Density ScoreMalik ANoch keine Bewertungen
- NCMC103 Prelims ReviewerDokument13 SeitenNCMC103 Prelims ReviewerVeronica ShaneNoch keine Bewertungen
- Maternal and Foetal Outcomes in Pregnancy With Gestational Thrombocytopenia: A Prospective Observational StudyDokument6 SeitenMaternal and Foetal Outcomes in Pregnancy With Gestational Thrombocytopenia: A Prospective Observational StudyIJAR JOURNALNoch keine Bewertungen
- Name: Strand, Grade & Section: - Maecy S. Paglinawan - STEM 12-15Dokument15 SeitenName: Strand, Grade & Section: - Maecy S. Paglinawan - STEM 12-15Maecy S. PaglinawanNoch keine Bewertungen
- Catalogo Libros Transfusion PDFDokument44 SeitenCatalogo Libros Transfusion PDFmeds1313Noch keine Bewertungen
- Freud and AnesthesiaDokument5 SeitenFreud and AnesthesiaRaluca LNoch keine Bewertungen
- Supliment Decembrie-2020 FinalDokument129 SeitenSupliment Decembrie-2020 FinalIrina IonescuNoch keine Bewertungen
- FieldworkDokument22 SeitenFieldworkLusungu S. LupenzaNoch keine Bewertungen
- Resultados SaludDignaDokument2 SeitenResultados SaludDignaAdriana RamosNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Unit 7 Reporting and RecordingDokument3 SeitenUnit 7 Reporting and RecordingZaidan YusufNoch keine Bewertungen
- High Yield Step 1 ImagesDokument65 SeitenHigh Yield Step 1 Imagesaditya mishraNoch keine Bewertungen
- Adenomiosis CX ConservadoraDokument12 SeitenAdenomiosis CX Conservadorajuan carlos pradaNoch keine Bewertungen
- Saprolegnia Diclina IIIA and S. Parasitica Employ Different Infection Strategies When Colonizing Eggs of Atlantic Salmon, Salmo Salar LDokument10 SeitenSaprolegnia Diclina IIIA and S. Parasitica Employ Different Infection Strategies When Colonizing Eggs of Atlantic Salmon, Salmo Salar LcamilaNoch keine Bewertungen
- L1.clinical ChemistryDokument37 SeitenL1.clinical Chemistrysini gangNoch keine Bewertungen
- Lowdermilk: Maternity & Women's Health Care, 10th EditionDokument12 SeitenLowdermilk: Maternity & Women's Health Care, 10th Editionvanassa johnson100% (1)
- Internal Medicine 1, Conrad FischerDokument35 SeitenInternal Medicine 1, Conrad Fischerdukelist566100% (3)
- Definition:: Pleural EffusionDokument4 SeitenDefinition:: Pleural EffusionGetom NgukirNoch keine Bewertungen
- Bekas SC 3xDokument22 SeitenBekas SC 3xpraburastraNoch keine Bewertungen
- Group WorkDokument19 SeitenGroup WorkSoumya Ranjan ParidaNoch keine Bewertungen
- 345-Article Text-1032-1-10-20180629Dokument4 Seiten345-Article Text-1032-1-10-20180629Regina AyediaNoch keine Bewertungen
- Endodontic Management of Mandibular Premolar With Two RootsDokument3 SeitenEndodontic Management of Mandibular Premolar With Two RootsJitender ReddyNoch keine Bewertungen
- المراجعة النهائية Final July EMSDokument293 Seitenالمراجعة النهائية Final July EMSAbdo MahfouzNoch keine Bewertungen
- STG 4thDokument1.239 SeitenSTG 4thFentahun workieNoch keine Bewertungen
- CRISIL Industry Report - HospitalDokument9 SeitenCRISIL Industry Report - Hospitalrahul.joisher2026Noch keine Bewertungen
- Kode Icd X Spesialistik FixDokument2 SeitenKode Icd X Spesialistik FixPuskesmas CipicungNoch keine Bewertungen
- THE BOWEL NOSODES Paterson BookDokument17 SeitenTHE BOWEL NOSODES Paterson BookShasta Triri100% (1)
- Garcia, Nehemiah B. BSN 2Y2-2A: Ncma 219 Rle Course Task # 2Dokument3 SeitenGarcia, Nehemiah B. BSN 2Y2-2A: Ncma 219 Rle Course Task # 2Mushy_ayaNoch keine Bewertungen
- Lab Ex 2 - Serial DilutionDokument2 SeitenLab Ex 2 - Serial DilutionMariel AbellezaNoch keine Bewertungen
- A) MarasmusDokument21 SeitenA) Marasmusrathai0% (1)
- Advanced Tung Style Acupuncture Vol. 2 - Obstetrics & Gynecology PDFDokument556 SeitenAdvanced Tung Style Acupuncture Vol. 2 - Obstetrics & Gynecology PDFnhung_nguyen_12260% (5)
- Pharmacology Test 1 Drug ListDokument20 SeitenPharmacology Test 1 Drug ListSHRIKANTNoch keine Bewertungen
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (378)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- Summary of Mary Claire Haver's The Galveston DietVon EverandSummary of Mary Claire Haver's The Galveston DietBewertung: 5 von 5 Sternen5/5 (1)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthVon EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthBewertung: 4 von 5 Sternen4/5 (6)