Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Fema Ics 200Dokument1 SeiteFema Ics 200api-455495817Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Fema Ics 100Dokument1 SeiteFema Ics 100api-455495817Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Nursing ShortageDokument6 SeitenThe Nursing Shortageapi-455495817Noch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Scholarly Capstone PaperDokument5 SeitenScholarly Capstone Paperapi-455495817Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Resume - Marium KhanDokument1 SeiteResume - Marium Khanapi-455495817Noch keine Bewertungen
- Background Results: Sarah E. Lade & Laurel J. Trainor Livelab, Mcmaster University, Ontario, CanadaDokument1 SeiteBackground Results: Sarah E. Lade & Laurel J. Trainor Livelab, Mcmaster University, Ontario, CanadaAnonymous GqwolA5kjaNoch keine Bewertungen
- Current Research Track ResidentsDokument5 SeitenCurrent Research Track ResidentsThusith WijayawardenaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Theraputic Counseling Intervention-BookDokument301 SeitenTheraputic Counseling Intervention-BookMiha Şi AtâtNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hypochondria 3 FormsDokument9 SeitenHypochondria 3 FormsYulianMitevNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- 10 1016@j Psychres 2018 06 033Dokument19 Seiten10 1016@j Psychres 2018 06 033sofiaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Comparație Între SCID 5 RV Și SCID 5 CVDokument3 SeitenComparație Între SCID 5 RV Și SCID 5 CVAdrianBelean100% (1)
- Mad in AmericaDokument13 SeitenMad in AmericaSadia AshrafNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Artikel Di Ios RDokument4 SeitenArtikel Di Ios RAriepputra PrawiraNoch keine Bewertungen
- SWD Aut19 NewsletterDokument27 SeitenSWD Aut19 NewsletterJuze DowdeeNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Stress Reading 1Dokument1 SeiteStress Reading 1HABLA BONITO LANGUAGE SCHOOL SCNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Essay ELADokument2 SeitenEssay ELAZuwaidah Ahmad SuhaimiNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- 5 Right-Brain Affect Regulation An Essential Mechanism of Development, Trauma, Dissociation, and Psychotherapy Allan N. SchoreDokument2 Seiten5 Right-Brain Affect Regulation An Essential Mechanism of Development, Trauma, Dissociation, and Psychotherapy Allan N. SchoreErika Olaechea GilNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Psychosocial NursingDokument21 SeitenPsychosocial NursingAngeline Angeles100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Association Between Video Gaming and Psychological FunctioningDokument11 SeitenThe Association Between Video Gaming and Psychological FunctioningALI RAZANoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 1989 The Revised Diagnostic Interview Zanarini1989Dokument9 Seiten1989 The Revised Diagnostic Interview Zanarini1989Cesar Cantarutti0% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Eye Movement Desensitization and Reprocessing EMDRDokument5 SeitenEye Movement Desensitization and Reprocessing EMDRSalem alarjaniNoch keine Bewertungen
- Palliative Care in Patients With Severe Mental Illness: Case 1Dokument3 SeitenPalliative Care in Patients With Severe Mental Illness: Case 1Cristian Vale VarelaNoch keine Bewertungen
- Psychiatry AnnGenPsychiatry 2007 Mousavi Suicide-Aggresion-Violence PosterDokument1 SeitePsychiatry AnnGenPsychiatry 2007 Mousavi Suicide-Aggresion-Violence PosterVictor Lopez SueroNoch keine Bewertungen
- Crack Powerpoint 3Dokument21 SeitenCrack Powerpoint 3api-285123736Noch keine Bewertungen
- Social Case WorkDokument53 SeitenSocial Case WorkAnonymous bvUE4d90% (29)
- Ximena Tovar Perez: CausesDokument3 SeitenXimena Tovar Perez: CausesXimena TovarNoch keine Bewertungen
- Appearance - Comparison RRLDokument9 SeitenAppearance - Comparison RRLKeen ZeahNoch keine Bewertungen
- Homeless Veterans 1Dokument2 SeitenHomeless Veterans 1api-317128838Noch keine Bewertungen
- Depresi Pada Seseorang Yang Mengalami PerceraianDokument4 SeitenDepresi Pada Seseorang Yang Mengalami PerceraianListyaningNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Electroconvulsive Therapy ManagementDokument32 SeitenElectroconvulsive Therapy ManagementNaeem KhanNoch keine Bewertungen
- PAI Score PiC PDFDokument7 SeitenPAI Score PiC PDFNatalia Figueroa Bravo0% (1)
- Kendler, Kenneth S. - Parnas, Josef - Philosophical Issues in Psychiatry - Explanation, Phenomenology, and Nosology-The Johns Hopkins University Press (2015)Dokument422 SeitenKendler, Kenneth S. - Parnas, Josef - Philosophical Issues in Psychiatry - Explanation, Phenomenology, and Nosology-The Johns Hopkins University Press (2015)Ziggy GonNoch keine Bewertungen
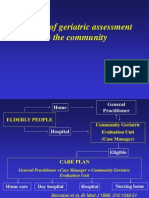
- The Use of Geriatric Assessment in The CommunityDokument16 SeitenThe Use of Geriatric Assessment in The Communityhendra2darmawanNoch keine Bewertungen
- Unani PsychiatryDokument6 SeitenUnani PsychiatryashfaqamarNoch keine Bewertungen
- Nursing Diagnosis: Acute ConfusionDokument4 SeitenNursing Diagnosis: Acute Confusionasmika danaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)