Das könnte Ihnen auch gefallen
- Dysarthria by Dr. Somesh MaheshwariDokument9 SeitenDysarthria by Dr. Somesh MaheshwariDr. Somesh MaheshwariNoch keine Bewertungen
- Enderby2013 Dysarthria Resumen PDFDokument9 SeitenEnderby2013 Dysarthria Resumen PDFPatricio RomeroNoch keine Bewertungen
- Aphasia, Apraxia, DysatrhriaDokument21 SeitenAphasia, Apraxia, Dysatrhriathosi1990Noch keine Bewertungen
- Assessment and Treatment of Linguistic Deficits PDFDokument96 SeitenAssessment and Treatment of Linguistic Deficits PDFJumraini TammasseNoch keine Bewertungen
- Hyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHyper-Salivation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Aphasia: Hana Nabila Ulfia 1102014118Dokument14 SeitenAphasia: Hana Nabila Ulfia 1102014118hana nabilaNoch keine Bewertungen
- Apraxia of SpeechDokument18 SeitenApraxia of SpeechfunkymonksnitzleNoch keine Bewertungen
- Differential Diagnosis DysarthriaDokument1 SeiteDifferential Diagnosis DysarthriaShruti KumarNoch keine Bewertungen
- AphasiaDokument29 SeitenAphasiaHannan FarooqNoch keine Bewertungen
- Speech and Language: Advances in Basic Research and PracticeVon EverandSpeech and Language: Advances in Basic Research and PracticeNoch keine Bewertungen
- Articulation DisorderDokument2 SeitenArticulation DisorderJustin Ahorro-DionisioNoch keine Bewertungen
- AphasiaDokument8 SeitenAphasiaapi-308647214Noch keine Bewertungen
- Methods of Speech Therapy Treatment For Stable Dysarthria A ReviewDokument14 SeitenMethods of Speech Therapy Treatment For Stable Dysarthria A ReviewDavid Trujillo BEatoNoch keine Bewertungen
- Language Aphasia: Lecture By: M.K. SastryDokument15 SeitenLanguage Aphasia: Lecture By: M.K. SastryAnonymous 5IUoLwGSdNoch keine Bewertungen
- Approach To The Patient With AphasiaDokument78 SeitenApproach To The Patient With Aphasiasurafel0% (1)
- Communication ProblemDokument85 SeitenCommunication ProblemHarshini SudharNoch keine Bewertungen
- UNIT I Phonological ProcessesDokument25 SeitenUNIT I Phonological ProcessesAurimar Hernández BarrientosNoch keine Bewertungen
- Final MSD Bringing It All Together Project 2Dokument7 SeitenFinal MSD Bringing It All Together Project 2api-557136848Noch keine Bewertungen
- (20838506 - Psychology of Language and Communication) Specific Language Impairment (SLI) - The Internet Ralli Campaign To Raise Awareness of SLIDokument6 Seiten(20838506 - Psychology of Language and Communication) Specific Language Impairment (SLI) - The Internet Ralli Campaign To Raise Awareness of SLIPaul AsturbiarisNoch keine Bewertungen
- ApraxiaDokument7 SeitenApraxiagemapesfNoch keine Bewertungen
- Post Stroke WritingDokument9 SeitenPost Stroke WritingAdi ParamarthaNoch keine Bewertungen
- Aphasia, Apraxia, and Agnosia AphasiaDokument7 SeitenAphasia, Apraxia, and Agnosia Aphasiasomebody_maNoch keine Bewertungen
- Natalie Brickner-Slp ResumeDokument1 SeiteNatalie Brickner-Slp Resumeapi-238387904Noch keine Bewertungen
- To Taste or Not To TasteDokument3 SeitenTo Taste or Not To TasteSpeech & Language Therapy in PracticeNoch keine Bewertungen
- pp2 Submission FormatDokument4 Seitenpp2 Submission Formatapi-314413672Noch keine Bewertungen
- GN Chapter 8 Communication DisordersDokument7 SeitenGN Chapter 8 Communication Disordersapi-316496339Noch keine Bewertungen
- 3.0 Speaking SkillsDokument41 Seiten3.0 Speaking Skillswan amirahNoch keine Bewertungen
- An Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisDokument6 SeitenAn Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisSaranya N MuthuNoch keine Bewertungen
- Types of Aac DevicesDokument19 SeitenTypes of Aac DevicesBatool Al-ferdowsiNoch keine Bewertungen
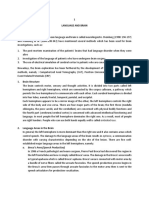
- 1 Language and Brain: A. Broca's Area (Speech Production)Dokument6 Seiten1 Language and Brain: A. Broca's Area (Speech Production)HasnaNoch keine Bewertungen
- Introduction To Language and Linguistics BIT10703 Ahmad Taufik Hidayah Bin AbdullahDokument5 SeitenIntroduction To Language and Linguistics BIT10703 Ahmad Taufik Hidayah Bin AbdullahMuhammad Ikhwan RosmanNoch keine Bewertungen
- Quick Aphasia Battery (QAB) : 1. Level of ConsciousnessDokument39 SeitenQuick Aphasia Battery (QAB) : 1. Level of ConsciousnessomeraNoch keine Bewertungen
- What Is DysarthriaDokument3 SeitenWhat Is DysarthriaAsnan Azis Fatoni100% (1)
- Approaches To Management of Stuttering (Piyush Malviya)Dokument11 SeitenApproaches To Management of Stuttering (Piyush Malviya)Piyush MalviyaNoch keine Bewertungen
- APHASIA++AND+COMMUNICATION PDF JsessionidDokument73 SeitenAPHASIA++AND+COMMUNICATION PDF Jsessionidami diyNoch keine Bewertungen
- Non-Speech Oro-Motor Exercises in Post-Stroke Dysarthria Intervention PDFDokument16 SeitenNon-Speech Oro-Motor Exercises in Post-Stroke Dysarthria Intervention PDFhgood1001Noch keine Bewertungen
- Motor Speech Skills in Down SyndromeDokument11 SeitenMotor Speech Skills in Down SyndromePaulaNoch keine Bewertungen
- Apraxia of SpeechDokument52 SeitenApraxia of Speechapi-3705274100% (3)
- ORLADokument10 SeitenORLACarol CoelhoNoch keine Bewertungen
- DysarthriaDokument2 SeitenDysarthriaBanjo VergaraNoch keine Bewertungen
- Comprehensive Handbook of Pediatric Audiology - (23 Behavioral Audiometry in Infants and Children)Dokument18 SeitenComprehensive Handbook of Pediatric Audiology - (23 Behavioral Audiometry in Infants and Children)Juliane NascimentoNoch keine Bewertungen
- Comcogtable 3 Summary All TestsDokument17 SeitenComcogtable 3 Summary All TestsanamariapobleteNoch keine Bewertungen
- 2014mshahandouts StoeckelDokument37 Seiten2014mshahandouts StoeckelAna Vogeley100% (1)
- Augmentative and Alternative CommunicationDokument19 SeitenAugmentative and Alternative Communicationt_areNoch keine Bewertungen
- 12724688Dokument98 Seiten12724688Melandes Tamiris100% (1)
- A at Motor SpeechDokument5 SeitenA at Motor SpeechNini JohannaNoch keine Bewertungen
- A Bright SPPARC.Dokument3 SeitenA Bright SPPARC.Speech & Language Therapy in PracticeNoch keine Bewertungen
- Cognitive Linguistic Assessment Protocol For Adults - Kannada Clap-KDokument47 SeitenCognitive Linguistic Assessment Protocol For Adults - Kannada Clap-KSureaka PonnusamyNoch keine Bewertungen
- Habla ClaraDokument14 SeitenHabla ClaraCristóbal Landeros TorresNoch keine Bewertungen
- Severity MatrixDokument1 SeiteSeverity MatrixCaroline100% (1)
- 2016 Duffy JR - Motor Speech Disorders Where Will We BeDokument6 Seiten2016 Duffy JR - Motor Speech Disorders Where Will We BeCarol TibaduizaNoch keine Bewertungen
- Learning Disabilities: by Priya Mary Paulose 1 Year M.SC NursingDokument51 SeitenLearning Disabilities: by Priya Mary Paulose 1 Year M.SC NursingPriya Mary PauloseNoch keine Bewertungen
- What Is AphasiaDokument4 SeitenWhat Is AphasiaValentina DubNoch keine Bewertungen
- Measuring Oral Health and Quality of LifeDokument172 SeitenMeasuring Oral Health and Quality of LifeCalin Dragoman100% (1)
- Management For Multiple HandicapDokument57 SeitenManagement For Multiple HandicapMSc Audio BNoch keine Bewertungen
- Speech & Language Therapy in Practice, Summer 2011Dokument36 SeitenSpeech & Language Therapy in Practice, Summer 2011Speech & Language Therapy in Practice100% (1)
- SB - Pediatrict Vocal NoduleDokument7 SeitenSB - Pediatrict Vocal NodulemediNoch keine Bewertungen
- Classification of Speech Disorders: December 2019Dokument21 SeitenClassification of Speech Disorders: December 2019Kirti Gunjikar0% (2)
- Dysarthria AssessmentDokument11 SeitenDysarthria AssessmentvviraaNoch keine Bewertungen
- Prescribing Information: (Methoxsalen, USP)Dokument9 SeitenPrescribing Information: (Methoxsalen, USP)Jeliny Bintan MaisuriNoch keine Bewertungen
- OHSS Case Presentation Discussion - Jindal IVF CHDDokument41 SeitenOHSS Case Presentation Discussion - Jindal IVF CHDJindal IVF ChandigarhNoch keine Bewertungen
- Nur 102Dokument3 SeitenNur 102Fretchel Grace Silverado MesaNoch keine Bewertungen
- Management of Infants BornDokument6 SeitenManagement of Infants BornDiana FlorezNoch keine Bewertungen
- Nutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 InfectionDokument13 SeitenNutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 Infectionmmbire@gmail.comNoch keine Bewertungen
- Etiologies of Failed Back Surgery SyndroDokument15 SeitenEtiologies of Failed Back Surgery SyndrowladjaNoch keine Bewertungen
- MCQ Question SheetDokument6 SeitenMCQ Question SheethappyhappylandNoch keine Bewertungen
- Original Contribution: The SHEZ StudyDokument9 SeitenOriginal Contribution: The SHEZ StudyRaúl AñariNoch keine Bewertungen
- PathophysiologyDokument13 SeitenPathophysiologyJan Phi LipNoch keine Bewertungen
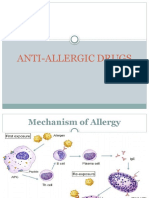
- Anti Allergic DrugsDokument18 SeitenAnti Allergic Drugsaamer niaziNoch keine Bewertungen
- 2017 PTMAZEiftDokument4 Seiten2017 PTMAZEiftAnindya DeNoch keine Bewertungen
- PUBlic Challenges An Extended Stay ASSIGN 1Dokument7 SeitenPUBlic Challenges An Extended Stay ASSIGN 1Areesha KaleemNoch keine Bewertungen
- Lapkas Marasmus JadiDokument48 SeitenLapkas Marasmus JadiRivhan FauzanNoch keine Bewertungen
- AAO Network GlaucomaDokument59 SeitenAAO Network Glaucomasafasayed100% (1)
- Spontaneous Intracerebral HaemorrhageDokument3 SeitenSpontaneous Intracerebral Haemorrhageselvie87Noch keine Bewertungen
- Sample ChapterDokument11 SeitenSample Chapter05 ANJALI PRAKASHNoch keine Bewertungen
- ESOFAGITISDokument13 SeitenESOFAGITISliliana delgadoNoch keine Bewertungen
- Health Optimizing Physical Education Module 2 DepedDokument4 SeitenHealth Optimizing Physical Education Module 2 Depedjudy sinsNoch keine Bewertungen
- PancretitisDokument44 SeitenPancretitisMohammad Husni BanisalmanNoch keine Bewertungen
- Glossary of Psychiatry WikipediaDokument153 SeitenGlossary of Psychiatry WikipediaAkio OzaragaNoch keine Bewertungen
- DashBoard Health SampleDokument1 SeiteDashBoard Health SampleAliChana1Noch keine Bewertungen
- Research On Fasting and Cancer TreatmentDokument9 SeitenResearch On Fasting and Cancer TreatmentMNoch keine Bewertungen
- Case Study About Type II Diabetes MellitusDokument82 SeitenCase Study About Type II Diabetes MellitusKristine YoungNoch keine Bewertungen
- Betadine GargleDokument1 SeiteBetadine GargleReemALMousawiNoch keine Bewertungen
- Congenital Cytomegalovirus Infection Management and OutcomeDokument20 SeitenCongenital Cytomegalovirus Infection Management and Outcomegomitas21Noch keine Bewertungen
- Management of Ludwig's AnginaDokument13 SeitenManagement of Ludwig's AnginaNahal HashirNoch keine Bewertungen
- Carcinoma Thyroid: Izzati Nurmaya Sari (1610029013) Supervisor: Dr. Syaiful Mukhtar, SP.B-KBDDokument24 SeitenCarcinoma Thyroid: Izzati Nurmaya Sari (1610029013) Supervisor: Dr. Syaiful Mukhtar, SP.B-KBDIzzati N. SariNoch keine Bewertungen
- Anatomy Liver FlukeDokument3 SeitenAnatomy Liver Flukeapi-295865391Noch keine Bewertungen
- 16/09/2015 1 Mujtaba AshrafDokument44 Seiten16/09/2015 1 Mujtaba Ashrafதீரன் சக்திவேல்Noch keine Bewertungen
- NR 325 Diabetes Power-Student Copy1118Dokument39 SeitenNR 325 Diabetes Power-Student Copy1118John MixerNoch keine Bewertungen