Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Endobronchial Ultrasound: Dr. Deepak Talwar India's Best PulmonologistDokument3 SeitenEndobronchial Ultrasound: Dr. Deepak Talwar India's Best PulmonologistMetro HospitalNoch keine Bewertungen
- Liver Transplantation in Adults - Patient Selection and Pretransplantation Evaluation - UpToDateDokument13 SeitenLiver Transplantation in Adults - Patient Selection and Pretransplantation Evaluation - UpToDatematteoNoch keine Bewertungen
- Siemens Acuson S1000-3000 ManualsDokument518 SeitenSiemens Acuson S1000-3000 Manualsmohammed100% (6)
- KODIGSDokument57 SeitenKODIGSRicky Abenir Ramos Jr.Noch keine Bewertungen
- BTS Sarcoidosis Clinical StatementDokument17 SeitenBTS Sarcoidosis Clinical StatementDarrin WiebeNoch keine Bewertungen
- Organizing Committee: AdvisorDokument22 SeitenOrganizing Committee: AdvisorAnggit PudjiastutiNoch keine Bewertungen
- Aortic StenosisDokument9 SeitenAortic StenosisecocardioNoch keine Bewertungen
- Company Profile: Touching Your Needs With Optimum SolutionsDokument4 SeitenCompany Profile: Touching Your Needs With Optimum SolutionsYasso DiamondNoch keine Bewertungen
- How To Interpret An Echocardiography Report (For The Non-Imager) ?Dokument12 SeitenHow To Interpret An Echocardiography Report (For The Non-Imager) ?VandeosNoch keine Bewertungen
- Alcoholic Cardiomyopathy - UpToDateDokument29 SeitenAlcoholic Cardiomyopathy - UpToDateAnca StanNoch keine Bewertungen
- (Mahesh Chandra) Objective Cardiology PDFDokument609 Seiten(Mahesh Chandra) Objective Cardiology PDFfajarNoch keine Bewertungen
- Luigi P. Badano, Roberto M. Lang, Denisa Muraru - Textbook of Three-Dimensional Echocardiography (2019, Springer International Publishing)Dokument367 SeitenLuigi P. Badano, Roberto M. Lang, Denisa Muraru - Textbook of Three-Dimensional Echocardiography (2019, Springer International Publishing)Nicoletta Orphanou100% (1)
- CLC 4960151208Dokument7 SeitenCLC 4960151208DoraNoch keine Bewertungen
- Cardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureDokument13 SeitenCardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureGian CarloNoch keine Bewertungen
- Perioperative Optimization of Patients With Neuromuscular Disorders Undergoing Scoliosis Corrective Surgery: A Multidisciplinary Team ApproachDokument9 SeitenPerioperative Optimization of Patients With Neuromuscular Disorders Undergoing Scoliosis Corrective Surgery: A Multidisciplinary Team ApproachZvonkitza CertanecNoch keine Bewertungen
- Complications of Mitral Stenosis in PregnancyDokument3 SeitenComplications of Mitral Stenosis in PregnancyJulissapenacNoch keine Bewertungen
- Pit IkaDokument40 SeitenPit IkaKharis FaridanNoch keine Bewertungen
- Medicine Long Cases - DR - PraveenDokument118 SeitenMedicine Long Cases - DR - Praveendileepa madurangaNoch keine Bewertungen
- Point-of-Care Ultrasound in The Intensive Care UnitDokument19 SeitenPoint-of-Care Ultrasound in The Intensive Care UnitJose ManuelNoch keine Bewertungen
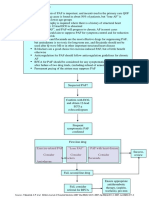
- Pathway DIAGNOSIS OF PAF FTRDokument1 SeitePathway DIAGNOSIS OF PAF FTRYoan Eka Putra PalilingNoch keine Bewertungen
- (Advances in Experimental Medicine and Biology 1133) Mieczyslaw Pokorski - Advances in Medicine and Medical Research-Springer International Publishing (2019) PDFDokument117 Seiten(Advances in Experimental Medicine and Biology 1133) Mieczyslaw Pokorski - Advances in Medicine and Medical Research-Springer International Publishing (2019) PDFHyper N0vaNoch keine Bewertungen
- 29 TB TTHL Danh Muc Sach Ngoai Van Tham KhaoDokument134 Seiten29 TB TTHL Danh Muc Sach Ngoai Van Tham Khaojames18b5Noch keine Bewertungen
- 64618-Cpd Units Application For October 14 2023Dokument30 Seiten64618-Cpd Units Application For October 14 2023prc.zamboanga.regulationcpdNoch keine Bewertungen
- Result Analysis Date: November 22, 2017 Conclusion: V. Laboratories and Diagnostic ExamsDokument7 SeitenResult Analysis Date: November 22, 2017 Conclusion: V. Laboratories and Diagnostic ExamsEllaine Joy Mesina PadizNoch keine Bewertungen
- Echo Pocket 2014Dokument18 SeitenEcho Pocket 2014abbouamine100% (2)
- Practical Perioperative Transesophageal EchocardiographyDokument349 SeitenPractical Perioperative Transesophageal Echocardiographyshirleyolivia100% (1)
- European J of Heart Fail - 2021 - Moura - Integration of Imaging and Circulating Biomarkers in Heart Failure A ConsensusDokument20 SeitenEuropean J of Heart Fail - 2021 - Moura - Integration of Imaging and Circulating Biomarkers in Heart Failure A Consensustotya91Noch keine Bewertungen
- Price List 2018-19 Latest ChangeDokument100 SeitenPrice List 2018-19 Latest ChangeJigar LadhavaNoch keine Bewertungen
- Test Bank For Surgical Technology Principles and Practice 6th Edition by Fuller DownloadDokument11 SeitenTest Bank For Surgical Technology Principles and Practice 6th Edition by Fuller DownloadCrystalDavisibng100% (17)
- Evolving Trends in Infective Endocarditis in A Developing Country: A Consequence of Medical Progress?Dokument9 SeitenEvolving Trends in Infective Endocarditis in A Developing Country: A Consequence of Medical Progress?Hassan Abdi JamaNoch keine Bewertungen