Das könnte Ihnen auch gefallen
- Neuroscience: Science of The BrainDokument60 SeitenNeuroscience: Science of The BrainInternational Brain Research Organization89% (76)
- Sample CCS-P Exam - (Multiple-Choice Questions)Dokument5 SeitenSample CCS-P Exam - (Multiple-Choice Questions)shyamsunder_nagula100% (1)
- Medical Terminology For Health Professions 7th Edition Ehrlich Solutions Manual 1Dokument24 SeitenMedical Terminology For Health Professions 7th Edition Ehrlich Solutions Manual 1leroy100% (50)
- Mortality & Death Audit FormatsDokument6 SeitenMortality & Death Audit FormatsAnindya BiswasNoch keine Bewertungen
- Adult Critical Care Nursing Knowledge & Skills ChecklistDokument7 SeitenAdult Critical Care Nursing Knowledge & Skills Checklistnorthweststaffing100% (3)
- Chronic Renal FailureDokument1 SeiteChronic Renal Failurejj_cuttingedges100% (2)
- CCSP Sample QuestionsDokument14 SeitenCCSP Sample Questionscarrie0871% (7)
- Myocardial Infarction And Cardiac DeathVon EverandMyocardial Infarction And Cardiac DeathErwin MarguliesBewertung: 1 von 5 Sternen1/5 (1)
- Penerapan PMKP RS Arjaty Daud 2022 UPDATEDokument15 SeitenPenerapan PMKP RS Arjaty Daud 2022 UPDATERUNI DARYANTI100% (1)
- Fluid and Electrolyte NCLEX EGEGGEDokument14 SeitenFluid and Electrolyte NCLEX EGEGGEELVINCE LACPAONoch keine Bewertungen
- Management of Life Threatening Asthma. Severe Asthma Series. CHEST 2022Dokument10 SeitenManagement of Life Threatening Asthma. Severe Asthma Series. CHEST 2022carla jazmin cortes rodriguezNoch keine Bewertungen
- Wound Debridement-FinalDokument3 SeitenWound Debridement-FinaljessicagrepoNoch keine Bewertungen
- OT Relevance RMTDokument12 SeitenOT Relevance RMTFredy RamoneNoch keine Bewertungen
- Disaster Mortality FormDokument1 SeiteDisaster Mortality FormThinaNoch keine Bewertungen
- Gambar MappingDokument9 SeitenGambar Mappingyana kristinaNoch keine Bewertungen
- D ReportDokument2 SeitenD ReportHihiNoch keine Bewertungen
- 2022 Care Plan 2Dokument9 Seiten2022 Care Plan 2api-601587526Noch keine Bewertungen
- High Risk Consent For PCIDokument1 SeiteHigh Risk Consent For PCISree Sowjanya PatibandlaNoch keine Bewertungen
- Stroke Form: Patient DataDokument6 SeitenStroke Form: Patient DataErikaMRSiaNoch keine Bewertungen
- Forrm 4aDokument4 SeitenForrm 4aJ.L. Jumbo XeroxNoch keine Bewertungen
- Critical Illness ClaimDokument7 SeitenCritical Illness ClaimIzzatt TazaliNoch keine Bewertungen
- Medical Forms A&BDokument6 SeitenMedical Forms A&BMarija CepuloNoch keine Bewertungen
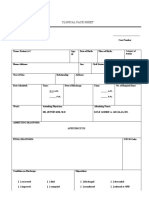
- Clinical Face Sheet: 8:13 A.M. - P.M. - A.M. - P.MDokument19 SeitenClinical Face Sheet: 8:13 A.M. - P.M. - A.M. - P.MKyle Audrie ArcalasNoch keine Bewertungen
- Center For Kidney Care Post TestDokument1 SeiteCenter For Kidney Care Post TestbladeemerNoch keine Bewertungen
- Cva BleedDokument99 SeitenCva BleedSHAMAE FAITH FARRENNoch keine Bewertungen
- Shekhawati Form - FDokument2 SeitenShekhawati Form - FArchit ChampanekarNoch keine Bewertungen
- Medical Terminology For Health Professions 7Th Edition Ehrlich Solutions Manual Full Chapter PDFDokument36 SeitenMedical Terminology For Health Professions 7Th Edition Ehrlich Solutions Manual Full Chapter PDFsusan.dean734100% (10)
- 3506 (From 2202) AlmadinDokument2 Seiten3506 (From 2202) AlmadinTirth PatelNoch keine Bewertungen
- Product Summary Flexi Vital CareDokument8 SeitenProduct Summary Flexi Vital CareJason Tan100% (2)
- 2020 CC CM and Pcs q4Dokument102 Seiten2020 CC CM and Pcs q4Rashiden MadjalesNoch keine Bewertungen
- Prelim ExaminationDokument5 SeitenPrelim ExaminationMary Grace AmbaNoch keine Bewertungen
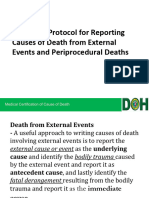
- Session 5-External EvantsDokument40 SeitenSession 5-External EvantsClarice ANoch keine Bewertungen
- Veterans Memorial Medical Center: Medical Records Unit CR-1 Records of HospitalizationDokument1 SeiteVeterans Memorial Medical Center: Medical Records Unit CR-1 Records of Hospitalizationclaverialc10Noch keine Bewertungen
- 2022 Care PlanDokument8 Seiten2022 Care Planapi-601587526Noch keine Bewertungen
- COVID-19 in Grade 4-5 Chronic Kidney Disease Patients: Case ReportDokument7 SeitenCOVID-19 in Grade 4-5 Chronic Kidney Disease Patients: Case ReportHendra DarmawanNoch keine Bewertungen
- Test Bank HemaDokument72 SeitenTest Bank HemaDesiree ArquisolaNoch keine Bewertungen
- Nejmoa 2206606Dokument10 SeitenNejmoa 2206606dipan diratuNoch keine Bewertungen
- BC Cardiac Catheterization Referral FormDokument1 SeiteBC Cardiac Catheterization Referral FormMr ShoaiBiNoch keine Bewertungen
- Fundamental of Nursing ExaminationDokument8 SeitenFundamental of Nursing ExaminationMary Grace Buscargas PolancosNoch keine Bewertungen
- SAFDAR The Prevalence of Short Peripheral Catheter-Related Blood Stream InfectionsDokument12 SeitenSAFDAR The Prevalence of Short Peripheral Catheter-Related Blood Stream InfectionsJohanna Brenke NarváezNoch keine Bewertungen
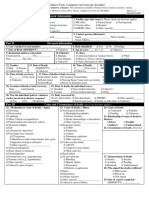
- Full ME Form PDFDokument1 SeiteFull ME Form PDFSubramanian SaravananNoch keine Bewertungen
- Cardiac ResuscitationDokument10 SeitenCardiac Resuscitationapi-3727533Noch keine Bewertungen
- On GK-HP2Dokument3 SeitenOn GK-HP2Kieu AnhNoch keine Bewertungen
- Mortality Aaudit FormatDokument6 SeitenMortality Aaudit FormatCOO TOP STARNoch keine Bewertungen
- Beige and Brown Aesthetic Group Project PresentationDokument73 SeitenBeige and Brown Aesthetic Group Project PresentationUDDE-E MARISABELNoch keine Bewertungen
- Phase 1Dokument15 SeitenPhase 1Dienizs LabiniNoch keine Bewertungen
- Unplanned Hospital Readmissions After Heartmate Ii ImplantationDokument9 SeitenUnplanned Hospital Readmissions After Heartmate Ii ImplantationBryan NguyenNoch keine Bewertungen
- Guidelines To Fill in Health Examination ReportDokument6 SeitenGuidelines To Fill in Health Examination ReportNurman HidayatNoch keine Bewertungen
- Weekly Test - Cardiovascular Emergencies Part 2Dokument5 SeitenWeekly Test - Cardiovascular Emergencies Part 2rajivsingal248Noch keine Bewertungen
- Cardiac Autotransplantation: Cooley Society 15th International SymposiumDokument5 SeitenCardiac Autotransplantation: Cooley Society 15th International SymposiumPeter Paul PascualNoch keine Bewertungen
- Revived Bcis2 TrialDokument10 SeitenRevived Bcis2 TrialSundaresan SankarNoch keine Bewertungen
- Sample: To: Accident and Emergency TeamDokument2 SeitenSample: To: Accident and Emergency TeamSabilatul AbidahNoch keine Bewertungen
- FiebreDokument5 SeitenFiebreIvana Daniela BelloNoch keine Bewertungen
- For Print - PADokument4 SeitenFor Print - PAJU DYNoch keine Bewertungen
- Asignatura: Ingles Tecnico Ii Ciclo: Vi Semestre Academico: 2020-2Dokument37 SeitenAsignatura: Ingles Tecnico Ii Ciclo: Vi Semestre Academico: 2020-2Jhon ArriagaNoch keine Bewertungen
- In Practice Sudden Cardiac Death Among Hemodialysis PatientsDokument12 SeitenIn Practice Sudden Cardiac Death Among Hemodialysis PatientsFreddy Shanner Chávez VásquezNoch keine Bewertungen
- Raksha New Pre-Authorization FormDokument1 SeiteRaksha New Pre-Authorization Formjigerpanchal0% (1)
- Perera Et Al 2023 Arrhythmia and Death Following Percutaneous Revascularization in Ischemic Left VentricularDokument10 SeitenPerera Et Al 2023 Arrhythmia and Death Following Percutaneous Revascularization in Ischemic Left VentriculardiegoiglesiasNoch keine Bewertungen
- Student Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415Dokument4 SeitenStudent Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415JohnNoch keine Bewertungen
- Lo0pkop (Mikoik0ojk0o Juojio NDokument2 SeitenLo0pkop (Mikoik0ojk0o Juojio NSrisachidanand ShuklaNoch keine Bewertungen
- Quiz Hospital DocumentationDokument5 SeitenQuiz Hospital DocumentationJessica EdiosNoch keine Bewertungen
- 5.+CR AriobimoDokument7 Seiten5.+CR AriobimoMia AmeliaNoch keine Bewertungen
- Liver Disease Questionnaire For Proposed Insured/OwnerDokument2 SeitenLiver Disease Questionnaire For Proposed Insured/OwnerSincerely ReynNoch keine Bewertungen
- 5 Medical-Surgical Nursing Questions (With Choices) ?: Report AbuseDokument6 Seiten5 Medical-Surgical Nursing Questions (With Choices) ?: Report Abusebhuvana4984Noch keine Bewertungen
- Mitral Valve Prolapse Research Jacc December 2022Dokument17 SeitenMitral Valve Prolapse Research Jacc December 2022Nox ÁtroposNoch keine Bewertungen
- Erosion of Cardiovascular Implantable Device: Conservative Therapy or Extraction?Dokument4 SeitenErosion of Cardiovascular Implantable Device: Conservative Therapy or Extraction?Randa TabbahNoch keine Bewertungen
- Clinical Face Sheet: - A.M. - P.M. - A.M. - P.MDokument7 SeitenClinical Face Sheet: - A.M. - P.M. - A.M. - P.MRenea Joy ArruejoNoch keine Bewertungen
- Temporary Permission Notification Connect Guide FundsDokument10 SeitenTemporary Permission Notification Connect Guide FundsUshaNoch keine Bewertungen
- Disease Management For Heart FailureDokument84 SeitenDisease Management For Heart FailureNational Pharmaceutical Council100% (7)
- (JTO (Civil) & JTO (Elect.) ) Under SRD For SC, ST & OBC Candidates in BSNL Will StartDokument5 Seiten(JTO (Civil) & JTO (Elect.) ) Under SRD For SC, ST & OBC Candidates in BSNL Will StartUshaNoch keine Bewertungen
- IDBI Assistant Manager Recruitment 2019.PDF-92Dokument20 SeitenIDBI Assistant Manager Recruitment 2019.PDF-92Subham GhoshNoch keine Bewertungen
- BARC Notification No 82Dokument6 SeitenBARC Notification No 82panditkapilNoch keine Bewertungen
- CEN - 02 - 2018 - Group DDokument36 SeitenCEN - 02 - 2018 - Group DRrb Jobs Alert86% (49)
- Administrative Law PDFDokument19 SeitenAdministrative Law PDFUshaNoch keine Bewertungen
- News Alerts and The Battle For The Lockscreen PDFDokument36 SeitenNews Alerts and The Battle For The Lockscreen PDFUshaNoch keine Bewertungen
- Sustainable Development in India: Perspectives by - Sunderlal BahugunaDokument10 SeitenSustainable Development in India: Perspectives by - Sunderlal BahugunajeevandohifodeNoch keine Bewertungen
- Ibps PoDokument27 SeitenIbps PoTopRankersNoch keine Bewertungen
- 2019 01 Notyfn Group I ServicesDokument19 Seiten2019 01 Notyfn Group I ServicesCyril PilligrinNoch keine Bewertungen
- CRbookDokument233 SeitenCRbookdeswitrigintaNoch keine Bewertungen
- Statutory Notifications For Nhs Bodies - Provider Guidance v6Dokument13 SeitenStatutory Notifications For Nhs Bodies - Provider Guidance v6UshaNoch keine Bewertungen
- 2019 01 Notyfn Group I ServicesDokument19 Seiten2019 01 Notyfn Group I ServicesCyril PilligrinNoch keine Bewertungen
- 2002 Cognitive DevDokument28 Seiten2002 Cognitive DevUshaNoch keine Bewertungen
- Cog TheoriesDokument73 SeitenCog Theoriesrenny wahyuniNoch keine Bewertungen
- Notification Preferences: Canvas NotificationsDokument16 SeitenNotification Preferences: Canvas NotificationsUshaNoch keine Bewertungen
- National Law Institute University, BhopalDokument14 SeitenNational Law Institute University, BhopalRohit Vijaya ChandraNoch keine Bewertungen
- ICSI Incorporation of Companies-8!8!2015Dokument168 SeitenICSI Incorporation of Companies-8!8!2015Lolitambika NeumannNoch keine Bewertungen
- Basic NeuroanatomyDokument35 SeitenBasic NeuroanatomyZahid GolandazNoch keine Bewertungen
- Basic NeuroanatomyDokument35 SeitenBasic NeuroanatomyZahid GolandazNoch keine Bewertungen
- Basic NeuroanatomyDokument35 SeitenBasic NeuroanatomyZahid GolandazNoch keine Bewertungen
- Piaget's Theory: Construct Their Own Knowledge On Their OwnDokument13 SeitenPiaget's Theory: Construct Their Own Knowledge On Their OwnAndra GabrielaNoch keine Bewertungen
- Chapter 3 2018Dokument12 SeitenChapter 3 2018UshaNoch keine Bewertungen
- Basic NeuroanatomyDokument35 SeitenBasic NeuroanatomyZahid GolandazNoch keine Bewertungen
- (World Health Organization) Neurological DisordersDokument232 Seiten(World Health Organization) Neurological DisordersAlina BreazuNoch keine Bewertungen
- Biological PsychologyDokument18 SeitenBiological PsychologyUshaNoch keine Bewertungen
- Formation of CompanyDokument18 SeitenFormation of CompanyPriti MishraNoch keine Bewertungen
- Guidelines JMIDokument17 SeitenGuidelines JMImunibfazalNoch keine Bewertungen
- The Canadian Etextbook of Eye MovementsDokument10 SeitenThe Canadian Etextbook of Eye Movementsrinitis123Noch keine Bewertungen
- African Swine FeverDokument4 SeitenAfrican Swine FeverJamaicah PattungNoch keine Bewertungen
- CancerDokument70 SeitenCancerapi-3735995100% (1)
- Meniscus Injuries: Uhuebor David Mbbs (Lagos)Dokument23 SeitenMeniscus Injuries: Uhuebor David Mbbs (Lagos)Uhuebor DavidNoch keine Bewertungen
- Reading Types of Nurses in HospitalDokument6 SeitenReading Types of Nurses in HospitalAlfa HamiseNoch keine Bewertungen
- Cholinergic System Model Questions & AnswersDokument45 SeitenCholinergic System Model Questions & AnswersDr.U.P.Rathnakar.MD.DIH.PGDHM100% (5)
- Missed Myocardial InfarctionDokument2 SeitenMissed Myocardial InfarctionHARITH RAJAH100% (1)
- OtosclerosisDokument46 SeitenOtosclerosisMariana CabralNoch keine Bewertungen
- Jurnal Forensik Trauma KimiaDokument5 SeitenJurnal Forensik Trauma Kimiaikram hanafiNoch keine Bewertungen
- Unit 6: Resistance of The Body To Infection: II. Immunity and AllergyDokument34 SeitenUnit 6: Resistance of The Body To Infection: II. Immunity and AllergyEsteban Tabares GonzalezNoch keine Bewertungen
- Acute Necrotizing Sinusitis Caused by Staphylococcus Lugdunensis 2011Dokument3 SeitenAcute Necrotizing Sinusitis Caused by Staphylococcus Lugdunensis 2011J Sebastian PeinadoNoch keine Bewertungen
- Travel NurseDokument1 SeiteTravel NursegiangNoch keine Bewertungen
- Types: There Is A Range Of, IncludingDokument15 SeitenTypes: There Is A Range Of, IncludingBhossneil Betonio LacadenNoch keine Bewertungen
- RL2 CCR Book March-2021-P117-118Dokument2 SeitenRL2 CCR Book March-2021-P117-118Judah ObengNoch keine Bewertungen
- Contoh Form IDODokument62 SeitenContoh Form IDOOki Vera UntariNoch keine Bewertungen
- Introduction and Evaluation of Pharmacovigilance For BeginnersDokument8 SeitenIntroduction and Evaluation of Pharmacovigilance For BeginnersShaun MerchantNoch keine Bewertungen
- Journal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDokument10 SeitenJournal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDR RISKA WAHYUNoch keine Bewertungen
- Brugada SyndromeDokument5 SeitenBrugada SyndromevitriaNoch keine Bewertungen
- COVID 19 FActsDokument1 SeiteCOVID 19 FActsKhzNoch keine Bewertungen
- Threats of Vector-Borne Zoonotic Disease in Europe: Dogs, Drosophilids, and Oriental Eye WormDokument3 SeitenThreats of Vector-Borne Zoonotic Disease in Europe: Dogs, Drosophilids, and Oriental Eye WormGustavo AndresNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaS R PanggabeanNoch keine Bewertungen
- Wurzel 2016Dokument8 SeitenWurzel 2016prolanis pkmmulyoharjoNoch keine Bewertungen
- Apollo Fertility IUI IVF Clinic and Dr. Lakshmi Krishna Leela GynecologistDokument6 SeitenApollo Fertility IUI IVF Clinic and Dr. Lakshmi Krishna Leela GynecologistPrabha SharmaNoch keine Bewertungen
- Lesson 2 - Administrative Order No. 2021-0037Dokument10 SeitenLesson 2 - Administrative Order No. 2021-0037Marjan CalzadoNoch keine Bewertungen