Das könnte Ihnen auch gefallen
- BMCPediatrics 2012 Prevalenceofbirthdefectsin Inner MongoliaDokument7 SeitenBMCPediatrics 2012 Prevalenceofbirthdefectsin Inner MongoliaErika PagalanNoch keine Bewertungen
- Prevalence of Congenital Anomalies in Neonates and Associated Risk Factors in A Tertiary Care Hospital in Eastern IndiaDokument7 SeitenPrevalence of Congenital Anomalies in Neonates and Associated Risk Factors in A Tertiary Care Hospital in Eastern Indiameylisa putri ayunandaNoch keine Bewertungen
- 9 JurnalDokument83 Seiten9 JurnalWanda AndiniNoch keine Bewertungen
- Maternal Malnutrition, Environmental Exposure During Pregnancy and The Risk of Non-Syndromic Orofacial CleftsDokument6 SeitenMaternal Malnutrition, Environmental Exposure During Pregnancy and The Risk of Non-Syndromic Orofacial CleftsFlórian JeffersonNoch keine Bewertungen
- 214 Research Papers Supporting The Vaccine/Autism LinkDokument180 Seiten214 Research Papers Supporting The Vaccine/Autism LinkGinger Taylor79% (291)
- A Study On Preterm Births During 2013-2015, Shiraz, Iran: Journal of Obstetrics and GynaecologyDokument6 SeitenA Study On Preterm Births During 2013-2015, Shiraz, Iran: Journal of Obstetrics and GynaecologyPangala NitaNoch keine Bewertungen
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsVon EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNoch keine Bewertungen
- Levels, Timing, and Etiology of Stillbirths in Sylhet District of BangladeshDokument10 SeitenLevels, Timing, and Etiology of Stillbirths in Sylhet District of Bangladeshayu_pieterNoch keine Bewertungen
- Risk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesDokument6 SeitenRisk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesRendra SyaniNoch keine Bewertungen
- EJNM-2021-81 Nyan Luqman AzizDokument9 SeitenEJNM-2021-81 Nyan Luqman AzizRista Afina WidyarkantiNoch keine Bewertungen
- 157 Research Papers Supporting The Vaccine Autism LinkDokument123 Seiten157 Research Papers Supporting The Vaccine Autism Linkdon fabNoch keine Bewertungen
- Congenital Nasolacrimal Duct Obstruction - Epidemiology and Risk FactorsDokument6 SeitenCongenital Nasolacrimal Duct Obstruction - Epidemiology and Risk FactorsLovely PoppyNoch keine Bewertungen
- Prevalence of The Cleft Lip and Palate Among Newborn Babies in Sulaimani Obstetrics and Gynecological HospitalDokument3 SeitenPrevalence of The Cleft Lip and Palate Among Newborn Babies in Sulaimani Obstetrics and Gynecological HospitalIOSRjournalNoch keine Bewertungen
- Recognizable Birth Defects Among Neonatal Admissions at A Tertiary Hospital in South Western Uganda: Prevalence, Patterns and Associated FactorsDokument13 SeitenRecognizable Birth Defects Among Neonatal Admissions at A Tertiary Hospital in South Western Uganda: Prevalence, Patterns and Associated FactorsInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Autismo EgiptoDokument8 SeitenAutismo EgiptoOvsd Vfsg SDNoch keine Bewertungen
- 521 2345 1 PB Converted 1Dokument14 Seiten521 2345 1 PB Converted 1prabuNoch keine Bewertungen
- Health Behaviors of Primigravida TeenagersDokument6 SeitenHealth Behaviors of Primigravida TeenagersAubrey UniqueNoch keine Bewertungen
- Risk Factors For Autism. Perinatal Factors Parental Psychiatric History and Socioeconomic StatusDokument10 SeitenRisk Factors For Autism. Perinatal Factors Parental Psychiatric History and Socioeconomic StatusJulio CesarNoch keine Bewertungen
- Factors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaDokument10 SeitenFactors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaInternational Journal of Current Innovations in Advanced Research100% (1)
- Under-Five Protein Energy Malnutrition Admitted at The University of Nigeria Teaching Hospital, Enugu: A 10 Year Retrospective ReviewDokument7 SeitenUnder-Five Protein Energy Malnutrition Admitted at The University of Nigeria Teaching Hospital, Enugu: A 10 Year Retrospective ReviewhfathiardiNoch keine Bewertungen
- Jurnal ObgynDokument10 SeitenJurnal ObgynUgi RahulNoch keine Bewertungen
- Birth Defect and It's Impact in Neonatal Health: A Review: Correspondence: DR Sharmin Afroze, Assistant ProfessorDokument10 SeitenBirth Defect and It's Impact in Neonatal Health: A Review: Correspondence: DR Sharmin Afroze, Assistant Professorw3wNoch keine Bewertungen
- Nigeria PDFDokument16 SeitenNigeria PDFrima weniNoch keine Bewertungen
- Nongenetic Risk Factors and CHD - Patel, Pediatr Cardiol, 2013Dokument22 SeitenNongenetic Risk Factors and CHD - Patel, Pediatr Cardiol, 2013Jacob DavisNoch keine Bewertungen
- Social Determinants of Health and Emergency Department Use Among Children With Sickle Cell DiseaseDokument4 SeitenSocial Determinants of Health and Emergency Department Use Among Children With Sickle Cell DiseaseLindsay CortrightNoch keine Bewertungen
- International Journal Health Research: Peer-Reviewed Online JournalDokument6 SeitenInternational Journal Health Research: Peer-Reviewed Online JournaldsNoch keine Bewertungen
- Sociodemographic Factors and Health Care Seeking Behaviours For Childhood IllnessesDokument7 SeitenSociodemographic Factors and Health Care Seeking Behaviours For Childhood IllnessesTengiz VerulavaNoch keine Bewertungen
- Halliday 1997Dokument8 SeitenHalliday 1997JohnnyNoch keine Bewertungen
- Risk Factors of Perinatal Asphyxia A Study at Al Diwaniya Maternity and Children Teaching HospitalDokument8 SeitenRisk Factors of Perinatal Asphyxia A Study at Al Diwaniya Maternity and Children Teaching HospitalRizky MuharramNoch keine Bewertungen
- 6 Nutrisi LBNDokument7 Seiten6 Nutrisi LBNRizalMarubobSilalahiNoch keine Bewertungen
- PIIS1472648318300427Dokument11 SeitenPIIS1472648318300427Thanh Binh TranNoch keine Bewertungen
- Case ControlDokument13 SeitenCase ControlririsNoch keine Bewertungen
- Contraception for the Medically Challenging PatientVon EverandContraception for the Medically Challenging PatientRebecca H. AllenNoch keine Bewertungen
- Maternal Mortality and Contributing Risk Factors: Kematian Maternal Dan Faktor-Faktor Risiko Yang MempengaruhinyaDokument6 SeitenMaternal Mortality and Contributing Risk Factors: Kematian Maternal Dan Faktor-Faktor Risiko Yang Mempengaruhinyanarto_chemz1013Noch keine Bewertungen
- 1564 3951 1 PBDokument5 Seiten1564 3951 1 PBsandy candyNoch keine Bewertungen
- ArticleDokument8 SeitenArticleAstrid Abrahams PakelNoch keine Bewertungen
- Lebanon - Congenital Anomalies Prevalence and Risk FactorsDokument7 SeitenLebanon - Congenital Anomalies Prevalence and Risk FactorsAbdelrhman WagdyNoch keine Bewertungen
- ASQ1Dokument14 SeitenASQ1janakaNoch keine Bewertungen
- Gha 9 28822Dokument8 SeitenGha 9 28822wulan wijayaNoch keine Bewertungen
- The Complex Aetiology of Cerebral PalsyDokument16 SeitenThe Complex Aetiology of Cerebral PalsyAileen MéndezNoch keine Bewertungen
- Autism RiskDokument14 SeitenAutism RiskAlina Topor Psi-MedicalNoch keine Bewertungen
- 20.ANGGUN NOVITA SARI 17321194066 Review JournalDokument4 Seiten20.ANGGUN NOVITA SARI 17321194066 Review JournalANGGUN NOVITA SARINoch keine Bewertungen
- International Journal of Pharmaceutical Science Invention (IJPSI)Dokument4 SeitenInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNoch keine Bewertungen
- Genetic Disorders and the Fetus: Diagnosis, Prevention, and TreatmentVon EverandGenetic Disorders and the Fetus: Diagnosis, Prevention, and TreatmentNoch keine Bewertungen
- Perinatalni I Prenatalni Uzroci AutizmaDokument8 SeitenPerinatalni I Prenatalni Uzroci AutizmaJohn SmithNoch keine Bewertungen
- Emery and Rimoin’s Principles and Practice of Medical Genetics and Genomics: Clinical Principles and ApplicationsVon EverandEmery and Rimoin’s Principles and Practice of Medical Genetics and Genomics: Clinical Principles and ApplicationsReed E. PyeritzNoch keine Bewertungen
- Anemia in Pregnancy in Malaysia: A Cross-Sectional Survey: Original ArticleDokument10 SeitenAnemia in Pregnancy in Malaysia: A Cross-Sectional Survey: Original ArticleThomson AffendyNoch keine Bewertungen
- Evaluation of The Child With Global Developmental DelayDokument14 SeitenEvaluation of The Child With Global Developmental DelayplaincircleNoch keine Bewertungen
- Depression Among Infertile Women in Gaza Strip PreDokument16 SeitenDepression Among Infertile Women in Gaza Strip Pregamal attamNoch keine Bewertungen
- Congenital Anomalies Among Newborn Babies in Felege Hiwot Comprehensive Specialized Referral Hospital, Bahir Dar, EthiopiaDokument8 SeitenCongenital Anomalies Among Newborn Babies in Felege Hiwot Comprehensive Specialized Referral Hospital, Bahir Dar, EthiopiaTadesse MuhammedNoch keine Bewertungen
- Jurnal Obgyn RimaDokument11 SeitenJurnal Obgyn RimaNetacoassyNoch keine Bewertungen
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsVon EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNoch keine Bewertungen
- Risk Factors in Early Life For Developmental Coordination Disorder: A Scoping ReviewDokument9 SeitenRisk Factors in Early Life For Developmental Coordination Disorder: A Scoping ReviewLaura RodriguezNoch keine Bewertungen
- 4 Ijeefusoct20174Dokument10 Seiten4 Ijeefusoct20174TJPRC PublicationsNoch keine Bewertungen
- BMC Public HealthDokument5 SeitenBMC Public HealthDag Eva SanthiNoch keine Bewertungen
- Birth Defects Research PaperDokument7 SeitenBirth Defects Research Paperjhwmemrhf100% (1)
- Congenital Malformations in The Newborn Population: A Population Study and Analysis of The Effect of Sex and PrematurityDokument6 SeitenCongenital Malformations in The Newborn Population: A Population Study and Analysis of The Effect of Sex and PrematuritydentsavvyNoch keine Bewertungen
- 33873-Article Text-121761-1-10-20170831Dokument6 Seiten33873-Article Text-121761-1-10-20170831AnggaNoch keine Bewertungen
- JurnalDokument18 SeitenJurnalEry ShaffaNoch keine Bewertungen
- JURNAL MomayyeziDokument14 SeitenJURNAL MomayyeziSeptianNoch keine Bewertungen
- Risk Factors Related To Omphalocele and GastroschisisDokument6 SeitenRisk Factors Related To Omphalocele and GastroschisisFahmiNoch keine Bewertungen
- Complete Summary: Guideline TitleDokument11 SeitenComplete Summary: Guideline TitleAndiTiwsNoch keine Bewertungen
- MenopuseDokument15 SeitenMenopuseAndiTiwsNoch keine Bewertungen
- GastroschisisDokument17 SeitenGastroschisisHerna WahyuniNoch keine Bewertungen
- Omphalocele and Gastroschisis in Newborns: Over 16 Years of Experience From A Single ClinicDokument4 SeitenOmphalocele and Gastroschisis in Newborns: Over 16 Years of Experience From A Single ClinicAndiTiwsNoch keine Bewertungen
- Effect of Perioperatif Management On Intraseluler Pressure During Gynecologycal Laparascopic Pelvic Surgery PDFDokument6 SeitenEffect of Perioperatif Management On Intraseluler Pressure During Gynecologycal Laparascopic Pelvic Surgery PDFAndiTiwsNoch keine Bewertungen
- In Vitro Fertilisation/intracytoplasmic Sperm Injection Beyond 2020Dokument7 SeitenIn Vitro Fertilisation/intracytoplasmic Sperm Injection Beyond 2020AndiTiwsNoch keine Bewertungen
- Glutamine in The Fetus and Critically Ill Low Birth Weight Neonate Metabolism and Mechanism of Action1Dokument8 SeitenGlutamine in The Fetus and Critically Ill Low Birth Weight Neonate Metabolism and Mechanism of Action1AndiTiwsNoch keine Bewertungen
- Obstetric Patient in ICU Prospective From & Teaching Hospital in Pakistan PDFDokument8 SeitenObstetric Patient in ICU Prospective From & Teaching Hospital in Pakistan PDFAndiTiwsNoch keine Bewertungen
- Fluid Therapi in Perioperative Setting A Clinical Review PDFDokument12 SeitenFluid Therapi in Perioperative Setting A Clinical Review PDFAndiTiwsNoch keine Bewertungen
- Glutamine in The Fetus and Critically Ill Low Birth Weight Neonate Metabolism and Mechanism of Action1Dokument8 SeitenGlutamine in The Fetus and Critically Ill Low Birth Weight Neonate Metabolism and Mechanism of Action1AndiTiwsNoch keine Bewertungen
- Glutamine Metabolism: Nutritional and Clinical SignificanceDokument5 SeitenGlutamine Metabolism: Nutritional and Clinical SignificanceAndiTiwsNoch keine Bewertungen
- Effect of Perioperatif Management On Intraseluler Pressure During Gynecologycal Laparascopic Pelvic Surgery PDFDokument6 SeitenEffect of Perioperatif Management On Intraseluler Pressure During Gynecologycal Laparascopic Pelvic Surgery PDFAndiTiwsNoch keine Bewertungen
- Glutamine Metabolism: Nutritional and Clinical SignificanceDokument5 SeitenGlutamine Metabolism: Nutritional and Clinical SignificanceAndiTiwsNoch keine Bewertungen
- Reducing Risk Birth DefectDokument4 SeitenReducing Risk Birth DefectAndiTiwsNoch keine Bewertungen
- Reducing Risk Birth DefectDokument4 SeitenReducing Risk Birth DefectAndiTiwsNoch keine Bewertungen
- Challenges of The WorkingDokument6 SeitenChallenges of The WorkingAndiTiwsNoch keine Bewertungen
- Not All Cases of NTD Can Prevented by Fetal DefectDokument8 SeitenNot All Cases of NTD Can Prevented by Fetal DefectAndiTiwsNoch keine Bewertungen
- Bookshelf NBK222075 PDFDokument271 SeitenBookshelf NBK222075 PDFAndiTiwsNoch keine Bewertungen
- Birth Defect Are PreventableDokument2 SeitenBirth Defect Are PreventableAndiTiwsNoch keine Bewertungen
- Next Step For Birth Defect and PreventionDokument15 SeitenNext Step For Birth Defect and PreventionAndiTiwsNoch keine Bewertungen
- Faq 165Dokument3 SeitenFaq 165maletta humphriesNoch keine Bewertungen
- Analysis of Factors Influencing Female InfertilityDokument12 SeitenAnalysis of Factors Influencing Female InfertilityAndiTiwsNoch keine Bewertungen
- Next Step For Birth Defect and PreventionDokument15 SeitenNext Step For Birth Defect and PreventionAndiTiwsNoch keine Bewertungen
- Review ISK Pada KEhamilanDokument9 SeitenReview ISK Pada KEhamilanAndiTiwsNoch keine Bewertungen
- Urinary Tract Infections in Pregnancy: Old and New Unresolved Diagnostic and Therapeutic ProblemsDokument11 SeitenUrinary Tract Infections in Pregnancy: Old and New Unresolved Diagnostic and Therapeutic ProblemsRestu SNoch keine Bewertungen
- Cluster HDC WKWKWKDokument2 SeitenCluster HDC WKWKWKAndiTiwsNoch keine Bewertungen
- Effects of Different Crystalloid Solutions On Hemodynamics, Peripheral Perfusion, and The Microcirculation in Experimental Abdominal SepsisDokument11 SeitenEffects of Different Crystalloid Solutions On Hemodynamics, Peripheral Perfusion, and The Microcirculation in Experimental Abdominal SepsisNurul Dwi LestariNoch keine Bewertungen
- Tehhhhhhhhhh UiDokument1 SeiteTehhhhhhhhhh UiAndiTiwsNoch keine Bewertungen
- Apush Exam Explained For 2017-18Dokument12 SeitenApush Exam Explained For 2017-18api-222665337Noch keine Bewertungen
- Making A Response EssayDokument3 SeitenMaking A Response EssayChris ZaynNoch keine Bewertungen
- Lesson Plan 2 Shel SilversteinDokument2 SeitenLesson Plan 2 Shel Silversteinapi-282739763Noch keine Bewertungen
- 15PDSC001 Theory, Policy and Practice of Development 2013Dokument2 Seiten15PDSC001 Theory, Policy and Practice of Development 2013Ana SolerNoch keine Bewertungen
- Accenture TestDokument16 SeitenAccenture TestKumar SahebNoch keine Bewertungen
- Weekly Lesson Plan English VI: 1 PartialDokument2 SeitenWeekly Lesson Plan English VI: 1 PartialPerla OlguinNoch keine Bewertungen
- Act 3395 TdwaDokument5 SeitenAct 3395 TdwaBryan PhamNoch keine Bewertungen
- Curriculum & Requirements-1Dokument2 SeitenCurriculum & Requirements-1KrezielDulosEscobarNoch keine Bewertungen
- Final PortfolioDokument175 SeitenFinal Portfolioflorence baliwang100% (9)
- Aro Guntur (Army Recruitment Rally at Police Parad Ground, Ongole From 03JUL 2019 TO - 15 JUL 2019)Dokument5 SeitenAro Guntur (Army Recruitment Rally at Police Parad Ground, Ongole From 03JUL 2019 TO - 15 JUL 2019)Anilkumar KumarNoch keine Bewertungen
- Listening Skill Language InstructionDokument2 SeitenListening Skill Language InstructionAinul MardhyahNoch keine Bewertungen
- Summary of AssessmentsDokument2 SeitenSummary of Assessmentsapi-401644862Noch keine Bewertungen
- Richard Keshen - Reasonable Self-EsteemDokument215 SeitenRichard Keshen - Reasonable Self-Esteemphilogos100% (1)
- Cape Caribbean Studies Syllabus 2013Dokument3 SeitenCape Caribbean Studies Syllabus 2013Kadek Mardika0% (3)
- Answer SheetDokument1 SeiteAnswer SheetJohn Paul M. Tagapan100% (1)
- Chemistry Internal AssessmentDokument12 SeitenChemistry Internal AssessmentRavindra Narayan Aher100% (1)
- Placid Vidya Vihar SR - Sec.School: How To Apply OnlineDokument2 SeitenPlacid Vidya Vihar SR - Sec.School: How To Apply OnlineLiz Tresa AntonyNoch keine Bewertungen
- Presented By: Mubashir Hassan Prekshya Panth Priyanka Rajbhandari Neelam Kr. Patel Neeraj SinghalDokument19 SeitenPresented By: Mubashir Hassan Prekshya Panth Priyanka Rajbhandari Neelam Kr. Patel Neeraj SinghalANURADHA CHHIPANoch keine Bewertungen
- HebbDokument16 SeitenHebbAndrés Pereyra RabanalNoch keine Bewertungen
- ArtefactsDokument4 SeitenArtefactsapi-377778524Noch keine Bewertungen
- Gpat 2013 Question Paper PatternDokument3 SeitenGpat 2013 Question Paper PatternReginaNoch keine Bewertungen
- Traducere Metodologie INSCRIERI LB - ENGL - 2017 2018 2Dokument27 SeitenTraducere Metodologie INSCRIERI LB - ENGL - 2017 2018 2Xaera412Noch keine Bewertungen
- WHLP Week 5 Practical Research 2Dokument2 SeitenWHLP Week 5 Practical Research 2Arwen Rae Nisperos67% (3)
- Right To T To Information Act ACT - 2005: Karnataka Institu Institute of Medical Sciences Hu Ences HubliDokument28 SeitenRight To T To Information Act ACT - 2005: Karnataka Institu Institute of Medical Sciences Hu Ences HubliAakash HoskotiNoch keine Bewertungen
- Writing Statement of PurposeDokument13 SeitenWriting Statement of Purposemismael1983100% (1)
- Dussertation Project On Byju's AppDokument62 SeitenDussertation Project On Byju's AppAnil NP naikNoch keine Bewertungen
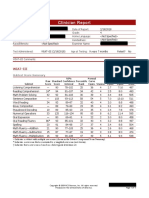
- Clinician Report: Wiat-IiiDokument5 SeitenClinician Report: Wiat-Iiiapi-395972621Noch keine Bewertungen
- Yolanda Paramitha ProceedingDokument6 SeitenYolanda Paramitha Proceedingyolanda paramithaNoch keine Bewertungen
- National Renowned EducatorsDokument17 SeitenNational Renowned EducatorshanshbeeNoch keine Bewertungen
- Dr. Babasaheb Ambedkar Marathwada University, Aurangabad LL.B (Three Year Degree Course) (I Semester) (CBCGSDokument2 SeitenDr. Babasaheb Ambedkar Marathwada University, Aurangabad LL.B (Three Year Degree Course) (I Semester) (CBCGSNishant ChaudhariNoch keine Bewertungen