Das könnte Ihnen auch gefallen
- Surgery 5 - Answers v1 (Wide)Dokument56 SeitenSurgery 5 - Answers v1 (Wide)Humzala BashamNoch keine Bewertungen
- David Perlmutter Focus Autoimmune PDFDokument23 SeitenDavid Perlmutter Focus Autoimmune PDFutpal_thakar100% (6)
- Other: Arterial VenousDokument3 SeitenOther: Arterial VenousMikaela Angeles NazarNoch keine Bewertungen
- Ouabain - The Optimal Solution For The Problem of Myocardial InfarctionDokument20 SeitenOuabain - The Optimal Solution For The Problem of Myocardial InfarctionredsbooksNoch keine Bewertungen
- Echocardiography in Fontan PhysiologyDokument30 SeitenEchocardiography in Fontan PhysiologyNavojit ChowdhuryNoch keine Bewertungen
- Occt651 - Occupational Profile Paper - FinalDokument20 SeitenOcct651 - Occupational Profile Paper - Finalapi-293182319Noch keine Bewertungen
- Withania Somnifera MonographDokument13 SeitenWithania Somnifera MonographVinita YadavNoch keine Bewertungen
- Multiple SclerosisDokument13 SeitenMultiple SclerosisGEETA MOHANNoch keine Bewertungen
- MRCS Essential ListDokument18 SeitenMRCS Essential ListMahmoud Selim100% (1)
- Acute Pulmonary Embolism Final YearDokument52 SeitenAcute Pulmonary Embolism Final YearUzma BanoNoch keine Bewertungen
- DR Franciscus Ginting - Sepsis PIN PAPDI Surabaya WS-051019-DikonversiDokument82 SeitenDR Franciscus Ginting - Sepsis PIN PAPDI Surabaya WS-051019-DikonversiDea LudjenNoch keine Bewertungen
- 4.penyembuhan LukaDokument52 Seiten4.penyembuhan LukaazisaaidrNoch keine Bewertungen
- Hepatopulmonary Syndrome - A Liver-Induced Lung Vascular DisorderDokument10 SeitenHepatopulmonary Syndrome - A Liver-Induced Lung Vascular DisorderFlavio FLores CruzNoch keine Bewertungen
- Full Text Brugada - AsmihaDokument4 SeitenFull Text Brugada - AsmihaNajla MasturaNoch keine Bewertungen
- UTMJ Case Reports VOL100 2 2023 3Dokument4 SeitenUTMJ Case Reports VOL100 2 2023 3Ariandindi AriandiNoch keine Bewertungen
- Application of The Continuous Autotransfusion System (CATS) To Prevent Transfusion-Related Hyperkalemia Following Hyperkalemic Cardiac Arrest in An Infant - A Case ReportDokument4 SeitenApplication of The Continuous Autotransfusion System (CATS) To Prevent Transfusion-Related Hyperkalemia Following Hyperkalemic Cardiac Arrest in An Infant - A Case Reportmaria bethania martins leiteNoch keine Bewertungen
- Usefulness of Hyponatremia in The Acute Phase of ST-Elevation Myocardial Infarction As A Marker of SeverityDokument6 SeitenUsefulness of Hyponatremia in The Acute Phase of ST-Elevation Myocardial Infarction As A Marker of SeverityJicko Street HooligansNoch keine Bewertungen
- Duty Report: Sunday, 27 May 2018Dokument17 SeitenDuty Report: Sunday, 27 May 2018HarisNoch keine Bewertungen
- 7756 PRDokument4 Seiten7756 PRThil4Noch keine Bewertungen
- Case Report - Deep Vein Thrombosis in Patient With Acute Heart Failure Due To Chemotherapy Induced CardiomyopathyDokument15 SeitenCase Report - Deep Vein Thrombosis in Patient With Acute Heart Failure Due To Chemotherapy Induced CardiomyopathyAbdurrohman IzzuddinNoch keine Bewertungen
- Lapkas VT RevisiDokument13 SeitenLapkas VT RevisiRannyNoch keine Bewertungen
- Atrial Myxoma (3g Hematology)Dokument25 SeitenAtrial Myxoma (3g Hematology)Vher John RamirezNoch keine Bewertungen
- Case Report: Possible Myocardial Tuberculosis Presenting With Congestive Heart Failure and Intracardiac ThrombusDokument11 SeitenCase Report: Possible Myocardial Tuberculosis Presenting With Congestive Heart Failure and Intracardiac ThrombusAbdurrohman IzzuddinNoch keine Bewertungen
- Case ReportDokument25 SeitenCase ReportFadhilah Amirah NasutionNoch keine Bewertungen
- Case Report Cushing SyndromeDokument8 SeitenCase Report Cushing SyndromeVivi DeviyanaNoch keine Bewertungen
- DR Franciscus Ginting - Sepsis PIN PAPDI SurabayaDokument82 SeitenDR Franciscus Ginting - Sepsis PIN PAPDI SurabayaSyahrul HamidNoch keine Bewertungen
- 1 PB PDFDokument4 Seiten1 PB PDFLe TrungNoch keine Bewertungen
- ST Elevation Myocard InfarkDokument30 SeitenST Elevation Myocard InfarkNancy Dwi Puspita100% (1)
- 2020 Refresher Course HematologyDokument50 Seiten2020 Refresher Course Hematologyshrwn.y.goNoch keine Bewertungen
- Wang Et Al 2018 Electrocardiographic Manifestations in Severe HypokalemiaDokument7 SeitenWang Et Al 2018 Electrocardiographic Manifestations in Severe HypokalemiaaisyahhelmadevithalibNoch keine Bewertungen
- Cerebral Infarction in Risk Factor of Adenoma and Symptomatic Aortic Stenosis Case Report and Literature Reviewp PDFDokument8 SeitenCerebral Infarction in Risk Factor of Adenoma and Symptomatic Aortic Stenosis Case Report and Literature Reviewp PDFFortune JournalsNoch keine Bewertungen
- Electrocardiograma en TóxicologiaDokument19 SeitenElectrocardiograma en TóxicologiaLaura GNoch keine Bewertungen
- Case Report DSSDokument3 SeitenCase Report DSSVivi DeviyanaNoch keine Bewertungen
- LLLT - Hypercholesterolemia (Animal Study)Dokument8 SeitenLLLT - Hypercholesterolemia (Animal Study)prettysia suvarlyNoch keine Bewertungen
- Acute Mesenteric Ischemia: A Challenging Diagnostic Disease-Four Cases Reports and Literature Review (AMI)Dokument10 SeitenAcute Mesenteric Ischemia: A Challenging Diagnostic Disease-Four Cases Reports and Literature Review (AMI)rahmatobineNoch keine Bewertungen
- Pleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterDokument46 SeitenPleural Diseases: Farhad Mazdisnian, MD, FCCP Pulmonary and Critical Care Medicine Va Long Beach Medical CenterderereyNoch keine Bewertungen
- A Case of Acute Tuberculous Pleuropneumonia in A Patient With Acute Lymphoblastic LeukemiaDokument9 SeitenA Case of Acute Tuberculous Pleuropneumonia in A Patient With Acute Lymphoblastic LeukemiaEasti EmoraNoch keine Bewertungen
- Heart MurmurDokument6 SeitenHeart MurmurYogendran MNoch keine Bewertungen
- Scorpion BiteDokument3 SeitenScorpion BiteNechifor BogdanNoch keine Bewertungen
- Critical Limits of Laboratory Results For Urgent Clinician NotificationDokument8 SeitenCritical Limits of Laboratory Results For Urgent Clinician NotificationMartesciuc VeraNoch keine Bewertungen
- Outcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac OperationDokument5 SeitenOutcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac OperationMuhammad RizqiNoch keine Bewertungen
- Case Report: An Unconscious Man With Profound Drug-Induced HypoglycaemiaDokument6 SeitenCase Report: An Unconscious Man With Profound Drug-Induced Hypoglycaemiagevowo3277Noch keine Bewertungen
- Tuberculous Pericarditis Leading To Cardiac Tamponade Importance of Screening Prior To ImmunosuppressionDokument3 SeitenTuberculous Pericarditis Leading To Cardiac Tamponade Importance of Screening Prior To ImmunosuppressionLink BuiNoch keine Bewertungen
- Pulmonary Oedema in A Hunting Dog: A Case Report: C.F. Agudelo, P. SchanilecDokument4 SeitenPulmonary Oedema in A Hunting Dog: A Case Report: C.F. Agudelo, P. SchanilecErlangga ReeNoch keine Bewertungen
- A Prothrombotic Thrombocytopenic Disorder Resembling Heparin-Induced Thrombocytopenia Following Coronavirus-19 VaccinationDokument8 SeitenA Prothrombotic Thrombocytopenic Disorder Resembling Heparin-Induced Thrombocytopenia Following Coronavirus-19 VaccinationJoseph Adinolfi Jr.100% (1)
- Two Cases of BRASH Syndrome: A Diagnostic Challenge: European Journal Internal MedicineDokument4 SeitenTwo Cases of BRASH Syndrome: A Diagnostic Challenge: European Journal Internal MedicineDesi MeliaNoch keine Bewertungen
- Anesthesia Monitoring Systems 1Dokument80 SeitenAnesthesia Monitoring Systems 1gnapikaNoch keine Bewertungen
- ELSO Interim Guidelines For Venoarterial.2Dokument18 SeitenELSO Interim Guidelines For Venoarterial.2BiancaPancuNoch keine Bewertungen
- GHHH HHHH HHHH K SssDokument4 SeitenGHHH HHHH HHHH K SssgabriellcvieiraNoch keine Bewertungen
- Mortality conference: ߡⰊשʑⅶⷪず कẤⵒ Reporter: CR⨀ᆙ Supervisor: CVS ⫯⸉Dokument42 SeitenMortality conference: ߡⰊשʑⅶⷪず कẤⵒ Reporter: CR⨀ᆙ Supervisor: CVS ⫯⸉劉彩屏Noch keine Bewertungen
- PDF 64982 2 10 20210118Dokument8 SeitenPDF 64982 2 10 20210118Marsya Yulinesia LoppiesNoch keine Bewertungen
- Final Myocarditis Associated With Influenzae A h1n1Dokument7 SeitenFinal Myocarditis Associated With Influenzae A h1n1Dr Gaurav SinghNoch keine Bewertungen
- Active Bleeding in Uremic Patients After Temporary Catheter Implantation Acase Report and Literature ReviewDokument3 SeitenActive Bleeding in Uremic Patients After Temporary Catheter Implantation Acase Report and Literature ReviewNiswaNoch keine Bewertungen
- Falla CardiacaDokument6 SeitenFalla CardiacaFelipeNoch keine Bewertungen
- Jurnal LED Internasional PDFDokument1 SeiteJurnal LED Internasional PDFJamaludin Winarhadi KusumoNoch keine Bewertungen
- Case Presentation On Copd - Shaik NazmaDokument29 SeitenCase Presentation On Copd - Shaik NazmaDeepikaNoch keine Bewertungen
- Lung Lobe Torsion in Seven Juvenile DogsDokument7 SeitenLung Lobe Torsion in Seven Juvenile DogsKelvinSueyzyNoch keine Bewertungen
- Cabot 2015Dokument9 SeitenCabot 2015Analia CortezNoch keine Bewertungen
- Recurrent Mycobacterium Tuberculosis Infection in Systemic Lupus Erythematosus Patient Case Report and ReviewDokument8 SeitenRecurrent Mycobacterium Tuberculosis Infection in Systemic Lupus Erythematosus Patient Case Report and ReviewpaulallenfileNoch keine Bewertungen
- Dr. Sunatrio - Management Hypovolemic ShockDokument59 SeitenDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNoch keine Bewertungen
- Ekg I PneumotoraksDokument4 SeitenEkg I Pneumotoraksstefan-13Noch keine Bewertungen
- Diagnosis and Management of ShockDokument26 SeitenDiagnosis and Management of Shockerwilli5Noch keine Bewertungen
- DIAGNOSTIC TEST Case StudyDokument14 SeitenDIAGNOSTIC TEST Case StudyAiner Anheca QuijadaNoch keine Bewertungen
- Lapkas JantungDokument25 SeitenLapkas JantungJuwita Valen RamadhanniaNoch keine Bewertungen
- Circulationaha 118 034075Dokument3 SeitenCirculationaha 118 034075Aldo Emir M. SarabiaNoch keine Bewertungen
- Clinical Handbook of Cardiac ElectrophysiologyVon EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverNoch keine Bewertungen
- Mehta 2013Dokument5 SeitenMehta 2013Gusti Ngurah PNoch keine Bewertungen
- Discovery and Development of Proton Pump Inhibitors: Hiroshi SatohDokument17 SeitenDiscovery and Development of Proton Pump Inhibitors: Hiroshi SatohGusti Ngurah PNoch keine Bewertungen
- Step 3:: Critically Appraising The Evidence: Statistics For TherapyDokument26 SeitenStep 3:: Critically Appraising The Evidence: Statistics For TherapyGusti Ngurah PNoch keine Bewertungen
- Allergic Contact DermatitisDokument5 SeitenAllergic Contact DermatitisGusti Ngurah PNoch keine Bewertungen
- Partial Lobar Collapse of Lung in Young Adult: A Case ReportDokument3 SeitenPartial Lobar Collapse of Lung in Young Adult: A Case ReportGusti Ngurah PNoch keine Bewertungen
- Weight-For-Length BOYS: Birth To 2 Years (Z-Scores)Dokument40 SeitenWeight-For-Length BOYS: Birth To 2 Years (Z-Scores)Gusti Ngurah PNoch keine Bewertungen
- Dr. Sameh Ahmad Muhamad Abdelghany Lecturer of Clinical Pharmacology Mansura Faculty of MedicineDokument52 SeitenDr. Sameh Ahmad Muhamad Abdelghany Lecturer of Clinical Pharmacology Mansura Faculty of MedicineAsep HrNoch keine Bewertungen
- Core Knowledge OrthopaedicsDokument2 SeitenCore Knowledge OrthopaedicsIamTineshNoch keine Bewertungen
- Hypokalemic Paralysis PDFDokument7 SeitenHypokalemic Paralysis PDFFanny SimaNoch keine Bewertungen
- Approach To Child With Fever: Liew Qian YiDokument33 SeitenApproach To Child With Fever: Liew Qian YinavenNoch keine Bewertungen
- Major Intra and Extracellular ElectrolytesDokument9 SeitenMajor Intra and Extracellular ElectrolytesJana BlueNoch keine Bewertungen
- AkiDokument20 SeitenAkiEnvhy AmaliaNoch keine Bewertungen
- Hypopituitarism: Dr. Rasikapriya First Year PaediatricsDokument34 SeitenHypopituitarism: Dr. Rasikapriya First Year PaediatricsReshu ThakuriNoch keine Bewertungen
- Medical Terminology Express A Short Course Approach by Body System 2nd Edition Gylys Test BankDokument13 SeitenMedical Terminology Express A Short Course Approach by Body System 2nd Edition Gylys Test Banksinapateprear4k100% (23)
- Lisinopril Prinivil Zestril)Dokument1 SeiteLisinopril Prinivil Zestril)ENoch keine Bewertungen
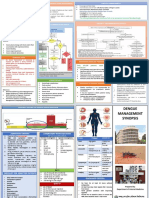
- Dengue Management Synopsis BSMMUDokument2 SeitenDengue Management Synopsis BSMMURakibk65Noch keine Bewertungen
- 45种严重疾病Dokument1 Seite45种严重疾病Kong Shi HaoNoch keine Bewertungen
- 403 Full PDFDokument10 Seiten403 Full PDFKuroto YoshikiNoch keine Bewertungen
- Group 1 QbankDokument10 SeitenGroup 1 QbankBatch ElysianNoch keine Bewertungen
- Pgi Physiology Exam: Your Email AddressDokument1 SeitePgi Physiology Exam: Your Email AddressCharlie65129Noch keine Bewertungen
- Imaging Features of Sarcoidosis On MDCT, FDG PET, and PET/CTDokument6 SeitenImaging Features of Sarcoidosis On MDCT, FDG PET, and PET/CTALE X RAYNoch keine Bewertungen
- OB - Hypertensive Disorders in PregnancyDokument6 SeitenOB - Hypertensive Disorders in PregnancyM MNoch keine Bewertungen
- Girls Who Masturbate in Early Infancy: Diagnostics, Natural Course and A Long-Term Follow-UpDokument5 SeitenGirls Who Masturbate in Early Infancy: Diagnostics, Natural Course and A Long-Term Follow-UpNurdin Aji IskandarNoch keine Bewertungen
- Key - 8th Grade Personal Consumer Health Study GuideDokument3 SeitenKey - 8th Grade Personal Consumer Health Study Guideapi-263456844Noch keine Bewertungen
- Salazar DsDokument4 SeitenSalazar DsDjayNoch keine Bewertungen
- Drug StudyDokument7 SeitenDrug StudySophia Rose Delos SantosNoch keine Bewertungen
- Bullous KeratopathyDokument2 SeitenBullous KeratopathyGershon HayfordNoch keine Bewertungen
- Eye & ENTDokument12 SeitenEye & ENTShandar SadafNoch keine Bewertungen
- Association Between Vitamin D and Systemic Lupus Erythematosus Disease Activity Index in Children and Adolescents - A Systematic Review and Meta-AnalysisDokument9 SeitenAssociation Between Vitamin D and Systemic Lupus Erythematosus Disease Activity Index in Children and Adolescents - A Systematic Review and Meta-AnalysiswatiNoch keine Bewertungen
- Convulsive Disorders: Presenters: Kabwe Chanda EliasDokument30 SeitenConvulsive Disorders: Presenters: Kabwe Chanda EliasHomeground entertainmentNoch keine Bewertungen