Das könnte Ihnen auch gefallen
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseVon EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNoch keine Bewertungen
- Oncology 101: Cancer BasicsDokument74 SeitenOncology 101: Cancer BasicsMary Rose Jose GragasinNoch keine Bewertungen
- Acute LeukemiasVon EverandAcute LeukemiasStefan H. FaderlNoch keine Bewertungen
- HPIM 20 OncologyDokument244 SeitenHPIM 20 OncologyapeachNoch keine Bewertungen
- Materi Prof Andri - Kanker ServiksDokument58 SeitenMateri Prof Andri - Kanker ServiksAnonymous WXQKCLL3Noch keine Bewertungen
- Article 1648703466Dokument6 SeitenArticle 1648703466Regla Mailyn Perez PerezNoch keine Bewertungen
- Healthy Choices Healthy Living: Talking About CancerDokument15 SeitenHealthy Choices Healthy Living: Talking About CancerStarboyNoch keine Bewertungen
- Case Study (Lung Cancer)Dokument17 SeitenCase Study (Lung Cancer)Jobelle Acena100% (1)
- Cancer PDFDokument65 SeitenCancer PDFhebert.mateoNoch keine Bewertungen
- Chronic Myeloid Leukemia: Chronic Phase Presenting As Extramedullary PresentationDokument6 SeitenChronic Myeloid Leukemia: Chronic Phase Presenting As Extramedullary PresentationOjas MahajanNoch keine Bewertungen
- Abstracts From Proceedings of The Society of Hematologic Oncology 2020 Annual MeetingDokument14 SeitenAbstracts From Proceedings of The Society of Hematologic Oncology 2020 Annual MeetingYakobus Antonius SobuberNoch keine Bewertungen
- Cardiactumors: Dylan V. MillerDokument31 SeitenCardiactumors: Dylan V. MillerAntonio FgNoch keine Bewertungen
- Kanker Growtf Factor Dan Tirosin KinaseDokument142 SeitenKanker Growtf Factor Dan Tirosin KinaseNovi KhamiliaNoch keine Bewertungen
- Acute Leukemia in ChildrenDokument15 SeitenAcute Leukemia in ChildrenSabrina JonesNoch keine Bewertungen
- An Introduction To CancerDokument42 SeitenAn Introduction To CancerAmjadRashidNoch keine Bewertungen
- Cancer Incidence in The Gaza Strip Facts & Figures 2015-2016Dokument13 SeitenCancer Incidence in The Gaza Strip Facts & Figures 2015-2016PressureserveNoch keine Bewertungen
- Neoplasia: Li Qun 2016.9Dokument61 SeitenNeoplasia: Li Qun 2016.9Osama SaidatNoch keine Bewertungen
- Study of RBC Histogram in Various AnemiasDokument15 SeitenStudy of RBC Histogram in Various Anemiasmsashmita555Noch keine Bewertungen
- Short Term Project Lab Report: Presented ByDokument22 SeitenShort Term Project Lab Report: Presented ByDebabrata SamantaNoch keine Bewertungen
- Clinical Aspect & Therapy of Acute LeukemiaDokument28 SeitenClinical Aspect & Therapy of Acute LeukemiaImtihanamiseNoch keine Bewertungen
- Kanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangDokument32 SeitenKanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangRakhmiNoch keine Bewertungen
- Kara CancerDokument45 SeitenKara CancerLinux MintNoch keine Bewertungen
- CBC Blood Test ExampleDokument3 SeitenCBC Blood Test Examplemazhar ehsanNoch keine Bewertungen
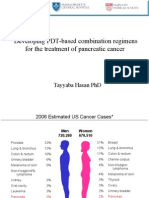
- Developing PDT-based Combination Regimens For The Treatment of Pancreatic CancerDokument33 SeitenDeveloping PDT-based Combination Regimens For The Treatment of Pancreatic CancerFirdosh DekhaiyaNoch keine Bewertungen
- Thyroid Cancer in Young Adults: Anita K. Ying, Winston Huh, Sarah Bottomley, Douglas B. Evans, and Steven G. WaguespackDokument17 SeitenThyroid Cancer in Young Adults: Anita K. Ying, Winston Huh, Sarah Bottomley, Douglas B. Evans, and Steven G. WaguespackBenny KurniawanNoch keine Bewertungen
- L13 OncologyDokument42 SeitenL13 OncologyHengkai NeoNoch keine Bewertungen
- Colorectal AdenomasDokument11 SeitenColorectal AdenomasMatias FlammNoch keine Bewertungen
- Introduction To Cancer Part2Dokument2 SeitenIntroduction To Cancer Part2jesperdomincilbayauaNoch keine Bewertungen
- Genetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceDokument74 SeitenGenetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceinakiNoch keine Bewertungen
- Breast Cancer ReviewDokument101 SeitenBreast Cancer ReviewByron Orlando Sanchez RomeroNoch keine Bewertungen
- 11-23-21 White Blood Cell DisordersDokument80 Seiten11-23-21 White Blood Cell DisordersdeNoch keine Bewertungen
- IasjDokument7 SeitenIasjismuNoch keine Bewertungen
- Advanced-Stagehodgkinlymphoma: by Joseph M. Connors, MDDokument5 SeitenAdvanced-Stagehodgkinlymphoma: by Joseph M. Connors, MDJOHN LOPERANoch keine Bewertungen
- Preventing and Reversing Cancer - The Absolute Health Integrative Oncology MethodDokument56 SeitenPreventing and Reversing Cancer - The Absolute Health Integrative Oncology MethodHalal Media MalaysiaNoch keine Bewertungen
- Acute Leukaemias Lecture-1Dokument39 SeitenAcute Leukaemias Lecture-1MarvellousNoch keine Bewertungen
- Kuliah 14.3 - Chronic Myeloid Leukemia (Dr. Ali Santosa)Dokument32 SeitenKuliah 14.3 - Chronic Myeloid Leukemia (Dr. Ali Santosa)Fikri UdinNoch keine Bewertungen
- Epidemiology of CancerDokument2 SeitenEpidemiology of CancerLilian LópezNoch keine Bewertungen
- Weledji 2020Dokument7 SeitenWeledji 2020Felipe CarmonaNoch keine Bewertungen
- 15 JMSCRDokument5 Seiten15 JMSCRbela melizaNoch keine Bewertungen
- Vii. Risk Factors For Multiple Myeloma: Increasing AgeDokument8 SeitenVii. Risk Factors For Multiple Myeloma: Increasing AgeHope SerquiñaNoch keine Bewertungen
- Study of Hematological Parameters in Patients With Non-Hematological Malignancies and Their Correlation With Stage of The DiseaseDokument7 SeitenStudy of Hematological Parameters in Patients With Non-Hematological Malignancies and Their Correlation With Stage of The DiseaseIJAR JOURNALNoch keine Bewertungen
- CancerDokument22 SeitenCancerPATRICK MARK FLORESNoch keine Bewertungen
- Thrombosis and Acute LeukemiaDokument6 SeitenThrombosis and Acute Leukemiaannisa edwarNoch keine Bewertungen
- Cervical CancerDokument22 SeitenCervical CancerfrankNoch keine Bewertungen
- Acute Lymphocytic LeukaemiaDokument100 SeitenAcute Lymphocytic LeukaemiaHan KethyanethNoch keine Bewertungen
- Acute Myeloid Leukemia With Myelodysplasia RelatedDokument6 SeitenAcute Myeloid Leukemia With Myelodysplasia RelatedAgus WiniNoch keine Bewertungen
- Acuteleukemia: Hayley Rose-Inman,, Damon KuehlDokument18 SeitenAcuteleukemia: Hayley Rose-Inman,, Damon KuehlJorge Tovar AvilaNoch keine Bewertungen
- 3.cancer AwarenessAndManagement SarahforOEDokument52 Seiten3.cancer AwarenessAndManagement SarahforOERustEdNoch keine Bewertungen
- 20 OncoDokument115 Seiten20 OncomichelleNoch keine Bewertungen
- Head and Neck Mucosal MelanomaDokument5 SeitenHead and Neck Mucosal MelanomaHAMIDNoch keine Bewertungen
- Cancer in Northern Queensland: CCQ Regional OfficeDokument4 SeitenCancer in Northern Queensland: CCQ Regional OfficeHNoch keine Bewertungen
- Pucat Dan Anemia Pada AnakDokument21 SeitenPucat Dan Anemia Pada AnakHerry WaraNoch keine Bewertungen
- Healthy Choices Healthy Living: Talking About CancerDokument15 SeitenHealthy Choices Healthy Living: Talking About CancerMila MarkovskaNoch keine Bewertungen
- Ejh 13396Dokument8 SeitenEjh 13396elyza putri novitasariNoch keine Bewertungen
- Acute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMDokument52 SeitenAcute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMJamilNoch keine Bewertungen
- Renal Cell CarcinomaDokument3 SeitenRenal Cell CarcinomaVon HippoNoch keine Bewertungen
- 1024 4076 1 PB 1Dokument11 Seiten1024 4076 1 PB 1Yulius TimotiusNoch keine Bewertungen
- Epidemiologie in EuropaDokument12 SeitenEpidemiologie in EuropaMonicaNoch keine Bewertungen
- Hepatic Metastasis From Colorectal CancerDokument11 SeitenHepatic Metastasis From Colorectal CancerApriani KudiNoch keine Bewertungen
- Final Research - LeukemiaDokument20 SeitenFinal Research - LeukemiaMohammed S. KhalilNoch keine Bewertungen
- The KDIGO AKI Guidelines: From 2011-2019Dokument38 SeitenThe KDIGO AKI Guidelines: From 2011-2019Andreas Agung KurniawanNoch keine Bewertungen
- Mantle CellDokument68 SeitenMantle CellAndreas Agung KurniawanNoch keine Bewertungen
- ICD BEDAH BARU Print SelesaiDokument12 SeitenICD BEDAH BARU Print SelesaiAndreas Agung KurniawanNoch keine Bewertungen
- ADHF Up To DateDokument25 SeitenADHF Up To DateAndreas Agung KurniawanNoch keine Bewertungen
- Pericarp & EndospermDokument1 SeitePericarp & EndospermAndreas Agung KurniawanNoch keine Bewertungen
- Analytical Exposition TextDokument3 SeitenAnalytical Exposition TextAndreas Agung KurniawanNoch keine Bewertungen
- Good BooksDokument16 SeitenGood BooksFbihansip bancel100% (1)
- Рецептор ба түүний төрлүүдDokument9 SeitenРецептор ба түүний төрлүүдАРСАЙNoch keine Bewertungen
- Recommended TextbooksDokument8 SeitenRecommended TextbooksShi Lin Lau0% (1)
- Science 6 - Week 4 - 2nd QuarterDokument5 SeitenScience 6 - Week 4 - 2nd QuarterHoneylet Alberto Castro ArilloNoch keine Bewertungen
- Medical CertificateDokument5 SeitenMedical CertificatePrasanna VenkatNoch keine Bewertungen
- Medind - Nic.in Icb t05 I5 Icbt05i5p445Dokument4 SeitenMedind - Nic.in Icb t05 I5 Icbt05i5p445Ester SibaraniNoch keine Bewertungen
- Sistem LimfatikDokument27 SeitenSistem LimfatikVani Taah GNoch keine Bewertungen
- Extension Worksheet - Option HDokument2 SeitenExtension Worksheet - Option HHellö PëachNoch keine Bewertungen
- ABG, CBC, BONE Marrow BiopsyDokument34 SeitenABG, CBC, BONE Marrow Biopsymarthonsilva123Noch keine Bewertungen
- Toxic A History of Nerve Agents From Nazi Germany To Putins Russia 1St Edition Edition Dan Kaszeta Download 2024 Full ChapterDokument23 SeitenToxic A History of Nerve Agents From Nazi Germany To Putins Russia 1St Edition Edition Dan Kaszeta Download 2024 Full Chaptermari.artrip178100% (9)
- Receptors Ion ChannelsDokument42 SeitenReceptors Ion ChannelsMd. Ahsan-Ul BariNoch keine Bewertungen
- Organic AcidsDokument25 SeitenOrganic Acidssatti_indianNoch keine Bewertungen
- Big Book of Kaiju #0Dokument17 SeitenBig Book of Kaiju #0Boracchio Pasquale100% (1)
- BIOM1050: Receptors, Neurons, Synapses & Nervous Systems Cell Communication & Receptor FamiliesDokument12 SeitenBIOM1050: Receptors, Neurons, Synapses & Nervous Systems Cell Communication & Receptor FamiliesmichelleNoch keine Bewertungen
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDokument12 SeitenAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991Noch keine Bewertungen
- B9780702031458000636 WebDokument13 SeitenB9780702031458000636 WebChristopher BermeoNoch keine Bewertungen
- Different Approaches in Pharmacological ResearchDokument3 SeitenDifferent Approaches in Pharmacological ResearcharcherselevatorsNoch keine Bewertungen
- Diffusion and Osmosis ESL 3Dokument27 SeitenDiffusion and Osmosis ESL 3Katie Isabella100% (1)
- Introduction To Lower Limb FinalDokument52 SeitenIntroduction To Lower Limb FinalRafique Ahmed100% (3)
- CPR Review Worksheet Ans KeyDokument9 SeitenCPR Review Worksheet Ans Keyapi-234803876Noch keine Bewertungen
- Chapter 12 - Cardiovascular EmergenciesDokument47 SeitenChapter 12 - Cardiovascular EmergenciesJunx TripoliNoch keine Bewertungen
- PT, Aptt, TTDokument44 SeitenPT, Aptt, TTswaraj sharmaNoch keine Bewertungen
- IB Biology Notes - 35 Transcription TranslationDokument2 SeitenIB Biology Notes - 35 Transcription TranslationJohn Philip D. NapalNoch keine Bewertungen
- DwsDokument27 SeitenDwsKunni MardhiyahNoch keine Bewertungen
- Overactivebladder 160426102342Dokument53 SeitenOveractivebladder 160426102342Tô Hoàng DũngNoch keine Bewertungen
- Herniated Nucleus PulposusDokument3 SeitenHerniated Nucleus PulposusroselleanneNoch keine Bewertungen
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDokument17 SeitenAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNoch keine Bewertungen
- Faradic Current: Prof - Dr. Mahmoud EwideaDokument75 SeitenFaradic Current: Prof - Dr. Mahmoud EwideaMahi GuptaNoch keine Bewertungen
- B.SC Botany Sem 1 To 6 2017Dokument72 SeitenB.SC Botany Sem 1 To 6 2017Jay ShethNoch keine Bewertungen
- CHAPTER 2 - Textbook ExerciseDokument8 SeitenCHAPTER 2 - Textbook ExerciseLeena HingNoch keine Bewertungen
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedBewertung: 4 von 5 Sternen4/5 (61)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)